
1Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Kowloon, Hong Kong
2Manchester Metropolitan University, Manchester, UK
Objective: To examine the feasibility and practicality of whole body vibration therapy for individuals with dystonic or spastic dystonic cerebral palsy.
Design: Pilot study.
Subjects: Children and adults with dystonic or spastic dystonic cerebral palsy.
Methods: Study participants received total body vibration therapy when standing still on a vibration platform for 3 bouts, duration 3-min, of vibration (20 Hz, 2 mm amplitude), 4 days per week for 4 weeks in addition to their usual therapy. All participants were assessed at baseline and completion of the study using the Gross Motor Function Measure Item Set, Timed Up and Go test, Barry-Albright Dystonia Scale, Edinburgh Visual Gait Score, and Pediatric Evaluation of Disability Inventory.
Results: Ten participants (mean age 18.60 years (standard deviation (SD) 14.68); 9 males, Gross Motor Function Classification System level II–IV) completed the study with more than 90% attendance rate. All participants tolerated the protocol with no adverse events.
Conclusion: The vibration treatment protocol was feasible and safe for all participants. With no significant differences found in all the outcome measures, future studies with more rigorous study designs are required before this intervention is recommended for this population group.
Key words: cerebral palsy; vibration; therapeutic use; physical therapy modalities; dystonia; balance; posture; gait.
Accepted Oct 11, 2019; published Oct 25, 2019
JRM-CC 2019; 2: 1000021
Correspondence address: Tamis W. Pin, Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Kowloon, Hong Kong. E-mail: tamis.pin@polyu.edu.hk
The aim of this study was to test the feasibility and practicality of whole body vibration therapy for people with dystonic or spastic dystonic cerebral palsy. Study participants received total body vibration therapy when standing still on a vibration platform for 3 bouts, duration 3-min, of vibration (20 Hz, 2 mm amplitude), 4 days per week for 4 weeks in addition to their usual therapy. All participants were assessed at baseline and completion of the study using various tests of balance, walking and daily activities. Ten participants (9 males, 1 female) age range 6–42 years, who could walk un-aided or with walking aids, completed the study, with more than 90% attendance rate. All participants tolerated the treatment with no problems. The vibration treatment was feasible and safe for all participants. No differences were found in any of the tests performed after the treatment. More studies are therefore needed before this treatment is recommended for people with dystonic or spastic dystonic cerebral palsy.
Whole body vibration therapy (WBVT) has recently been used as a neuro-modulation intervention for individuals with various neurological disorders (1, 2). In WBVT, the user stands stationary or performs specific dynamic movements on a platform providing vibrations from a few Hz to 50 Hz (Hz represents the number of complete vertical or sinusoidal movement cycles per s) (3). It is believed that the vibrations stimulate the alpha-motor neurones within the muscle spindles, eliciting the tonic vibration reflex. This reflex then induces voluntary muscle contractions, consequently increasing muscle strength (2, 4–6). The vibrations are also believed to stimulate peripheral mechanoreceptors and, if applied repeatedly, may induce neuroplasticity via somatosensory and motor pathways (7). It is also considered that the vibration may increase neural drive to the muscles to recruit previously inactive motor units, further enhancing muscle contractions (3).
Cerebral palsy (CP) is one of the most common childhood movement disorders, affecting approximately 2.5 per 1,000 live-births (8). The non-progressive brain damage in CP frequently results in hypertonia, poor motor control and muscle weakness (8). Over 80% of individuals with CP have spasticity, i.e. velocity-dependent resistance in their limbs (9). A smaller group of individuals with CP have dystonia, in which muscle tone varies between hypotonia and hypertonia, resulting in twisted postures, repetitive involuntary movements and distorted voluntary movements (10, 11). Individuals with mixed spasticity and dystonia are not uncommon (10). Individuals with CP are commonly classified using the 5-level Gross Motor Function Classification System (GMFCS) according to their functional abilities (12). GMFCS levels I and II refer to those who are able to ambulate independently without walking aids, but have limitations in advanced gross motor skills, such as running and jumping. Individuals of GMFCS level III rely on mobility aids for ambulation. GMFCS level IV refers to those who ambulate only with walking aids and manual assistance and GMFCS level V to those with totally dependent mobility (12).
If WBVT was able to stimulate the muscle spindles and elicit consistent muscle contractions, this would be advantageous for individuals with CP of GMFCS levels III or below who have limited motor ability to perform the same amount of regular exercises as their peers without CP. Research into the use of WBVT for children with CP has shown positive results on gross motor function, balance and muscle strength, but mainly for children of GMFCS levels I and II (1, 13). The majority of past studies in this area that yielded positive results required the study participants to perform simple exercises on the vibration platform as part of the intervention (1, 13). This is likely to be too demanding for those of GMFCS levels III or IV and those with poor motor control due to dystonia. Positive preliminary results of WBVT in improving functional skills and balance have been demonstrated in children and young adults with spastic CP of GMFCS levels III or IV using static standing on the vibration platform (14). Focal vibration has been shown to improve musician’s dystonia (2), but, as far as we know, no study has used WBVT on individuals with dystonic or spastic dystonic CP. It is not known if the claimed positive effects of using WBVT on individuals with spastic CP will be replicated in those with dystonic or spastic dystonic CP.
The aim of this pilot study was to explore this knowledge gap and make a preliminary examination of the effect of a 4-week static standing WBVT programme (14) on children and young adults with dystonic or spastic dystonic CP in terms of muscle tone, balance and functional motor abilities. The specific objectives were:
As a sample size calculation is not usually required for pilot studies (15), a convenience sample of 10 individuals aged between 6 and 45 years was targeted. This broad age range, with no limitation on GMFCS level, allowed examination of the feasibility of WBVT on a wide spectrum of this population group.
The inclusion criteria were participants: (i) with a diagnosis of CP; (ii) with presence of dystonia; (iii) able to stand for 3 min independently or with own hand support on rails; (iv) able to understand simple instructions; and (v) able to tolerate clinical examination.
The exclusion criteria were specific to WBVT and were participants: (i) with bone fracture 8 weeks prior to enrolment to the present study, or with acute thrombosis, muscle or tendon inflammation, renal stones, discopathy or arthritis, as reported by the participants and/or their parent/guardian; (ii) with metal implants in their spine or lower limbs; (iii) using anabolic agents or growth hormone for at least 1 month, within 3 months prior to enrolment into the present study; and (iv) being pregnant.
The presence of dystonia in the participants was first confirmed using the Hypertonia Assessment Tool (HAT) (16, 17) by the first author (TWP). The HAT is a reliable and valid clinical tool to confirm the presence of dystonia in individuals with CP (16). It consists of 7 items (2 on spasticity, 2 on rigidity and 3 on dystonia), scored using either 0 (absent) or 1 (present). A positive score of at least 1 item of the subgroup confirms the presence of hypertonia and the presence of items from more than 1 subgroup indicates mixed tone (16). Only those participants in whom dystonia or mixed tone was confirmed would be included in this study.
The study participants received the WBVT when standing still on the Galileo Med L Plus model 2000 (Novotech Medical GmbH, Germany), wearing their usual clothing and footwear: WBVT was provided in addition to their usual therapy programme. The WBVT intervention sessions consisted of 3 bouts, of 3-min-on and 3-minute-off , vibration (20 Hz, peak-to-peak amplitude of 2 mm) (14). Appendix I shows the gradual progression of the vibration parameters to the desired level so as to allow the study participants to become accustomed to the intense sensory stimulation from the vibration. The intervention took place on 4 days per week for 4 weeks.
All participants were assessed at baseline and at completion of the study by the first author using the following outcome measures:
Gross Motor Function Measure (GMFM-66) Item Set (IS) (18): a validated and reliable assessment of gross motor function in lying, sitting, 4-point kneeling, high kneeling and standing positions for individuals with CP (19). The GMFM-66 IS is a condensed version of the GMFM 66 that has been developed for research purposes (18). The total score is an estimate of the child’s gross motor function (18).
Timed Up and Go (TUG): this test assesses balance and mobility in a functional context where the participant stands up from a chair, walks for 5 m, returns and sits down (20, 21). The duration to complete this task was recorded.
Barry-Albright Dystonia Scale (BADS): this tests the severity of dystonia present in the eyes, mouth, neck, trunk and each upper and lower extremity (0 represents absence of dystonia to 4 represents severe dystonia present more than 50% of the time, and/or dystonia preventing any movements) (22).
Edinburgh Visual Gait Score (23, 24): examines the walking pattern for those independent walkers with or without walking aid. A total of 17 items in foot (5 items), knee (2 items), hip (1 item), pelvis (2 items) and trunk (2 items) is scored 0 (normal), 1 or 2 (severe deviation from normal). The sum of the scores of the 2 lower limbs was used for those with bilateral CP and the score of the affected lower limb for those with unilateral CP.
A validated Chinese version of the Pediatric Evaluation of Disability Inventory (PEDI) (25, 26) assesses functional capacities in the domains of daily activities (73 items) and mobility (59 items). A total score of each domain was recorded (0=”unable” and 1=”able”).
Visual analogue scales (VAS scores) were used to assess (i) any discomfort; and (ii) the degree of relaxation felt in the body associated with the intervention. The scale ranged from 0 (no discomfort/extreme “stiffness” felt in body) to 10 (extreme discomfort/extreme “loosening” felt in body), as reported by the study participants, along with any additional subjective comments they wished to make.
Due to the small sample size, non-parametric Wilcoxon signed-rank test was used to compare the results before and after the WBVT. The statistical significance level was set at p < 0.05.
Ethical approval was granted from the affiliated University of the first, third and fourth authors. An informed consent form was signed by participants over 18 years old, or by their parents/guardians for participants under 18 years old. The study was registered in ClinicalTrials.gov (NCT03779308).
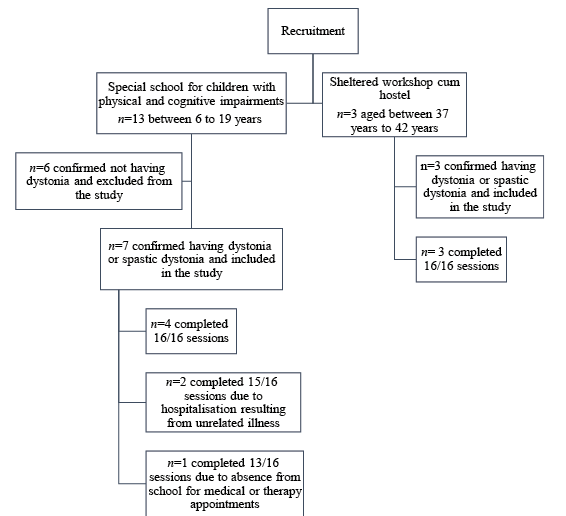
Thirteen participants were recruited from a special school for students with physical and cognitive impairments. Seven of these students were confirmed to have dystonic or spastic dystonic CP and were included in the study (mean age 9.86 years (standard deviation (SD) 4.85); 6 males, 85.7%). Three participants were screened and recruited from a sheltered workshop cum hostel (mean age 39.00 years (SD 2.65); 3 males, 100%) (Fig. 1). Table I shows the characteristics of the study participants. The majority of participants functioned at GMFCS level II or III (n = 8, 80%).
Fig. 1. Participant flowchart.
Table I. Characteristics of study participants
A physical therapist (4th author, NCP) provided the WBVT to all the study participants at their respective recruitment sites. The attendance rate of the study participants was 96.89% (SD 6.05). The greatest number of missed intervention sessions was 3 out of 16 sessions for one participant (DYS007, Fig. 1). Seven participants completed all 16 sessions. No adverse event was reported for any participant. All participants coped well with the protocol, and the physical therapist had no difficulty in delivering the on-site programme.
The performance of the study participants is shown in Table I and graphically in Fig. 2. The Wilcoxon signed-rank test showed no significant difference in any of the outcome measures. The mean VAS score in discomfort was 0.43 (SD 0.41) and 6.64 (SD 1.00) in the degree of relaxation felt in the body. All participants reported feeling very relaxed after the WBVT and approximately half of the participants reported “tiredness” in their legs after the intervention session.
Fig. 2. Graphs of study results. GMFM-66: Gross Motor Function Measure 66 Item Set; PEDI: Pediatric Evaluation of Disability Inventory.
This pilot study examined the feasibility of an adapted WBVT protocol for children and adults with moderate severity of dystonic or spastic dystonic CP. The study also investigated any trends towards change in functional abilities, gait pattern and muscle tone in the participants post-intervention.
Feasibility of the intervention protocol
The majority of WBVT interventions reported previously have required participants to perform simple exercises, e.g. mini-squats or lunges, on the vibration platform. This poses a great challenge for individuals with dystonic or spastic dystonic CP or for those with GMFCS levels III or below who do not have adequate motor control to perform these precise movements. However, these individuals are most vulnerable to poor muscle strength and motor function as a consequence of their greatly compromised mobility (4, 5), and thus the present study investigated the feasibility of static standing on the vibration platform with both knees in slight flexion and with hand support if needed. This protocol (Appendix I) was less demanding and has previously been proven to be feasible and safe for children and adults with spastic CP of GMFCS levels III or IV (14). Similar to our previous study on individuals with spastic CP, the participants in the present study tolerated the intervention well, missing sessions only due to previously scheduled appointments or unrelated illness. No adverse event was reported. These findings suggest that the present protocol of the WBVT was feasible and safe for the study participants across the wide age range and in routine clinical settings, thus fulfilling our primary objective.
With respect to trends in changing function, gait and muscle tone, the current study did not reveal any positive or negative trends in this 4-week WBVT programme. We believe that these insignificant study results may, in part, be due to the way in which WBVT influences muscle tone. Studies have shown that WBVT can inhibit the stretch reflex and the Hoffman-reflex, leading to positive results in reducing spasticity in patients post-stroke and with spinal cord injuries (2, 3). Our study participants had pre-dominant dystonia in their clinical presentation, which may explain the absence of change in the BADS score, an outcome measure that only assesses dystonia. For those participants presenting with spastic dystonia, it is possible that reduction in spasticity may have contributed to their improvement in gross motor function (e.g. DYS007), balance (e.g. DYS002) or walking pattern (e.g. DYS003). However, some participants may have been reliant on their extensor spasticity to stand, transfer between positions and walk (27, 28) and any reduction in spasticity might hamper their gross motor function (e.g. GMFM-66 IS of DYS008, TUG of DYS001 and EVGS of DYS005). It has been argued that the excessive movements of dystonia may be due to the loss of inhibition of undesired movements, rather than loss of excitation of desired movements (29). If this is so, then it is possible that the excitatory mechanism of WBVT on muscle spindles may have aroused the inhibitory pathway of undesired movements: thus only those participants with dominant dystonia would show positive results. This speculation can only be verified with future studies with more homogeneous study participants.
The current study also found that, overall, the results of the PEDI were contradictory to the results of other outcome measures. The PEDI is a questionnaire to assess functional abilities in self-care and mobility: it is answered by parents for child participants and by the adult participants in person. At present, we are unable to explain the underlying reason for this discrepancy.
Study limitations
This pilot study had a small sample size and a low level of study design. A possible learning effect may have occurred for the repeat tests at 4 weeks, and all tests were performed by only one examiner. However, the primary focus of this study was to ascertain the feasibility of the WBVT programme, and this was achieved successfully. WBVT for 4 weeks is a relatively short duration compared with previous studies (1, 13), but our primary aim was to examine the feasibility of WBVT for individuals with this sub-group of CP. Future studies with long study duration may be required to evaluate the benefits of WBVT for individuals with dystonic or spastic dystonia CP.
Conclusion
The results of the current pilot study have shown that the proposed static standing WBVT treatment protocol is feasible, safe and acceptable for children and adults with dystonia or spastic dystonia. In this small study, the treatment effect using this intervention appeared to be unpredictable for individual participants. Until future studies with more rigorous study designs, larger samples and longer study duration are conducted, there is no evidence to support the use of this intervention for this population group.
The authors would thank all the study participants and the staff at the SAHK Erik Kvan Workshop and Hostel and the Hong Kong Christian Services Pui Oi School.
This study was fully financed by The Hong Kong Polytechnic University internal research fund granted to Dr Tamis W. Pin.
The authors have no conflicts of interest to declare.
Appendix I. Intervention protocol for the present study


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize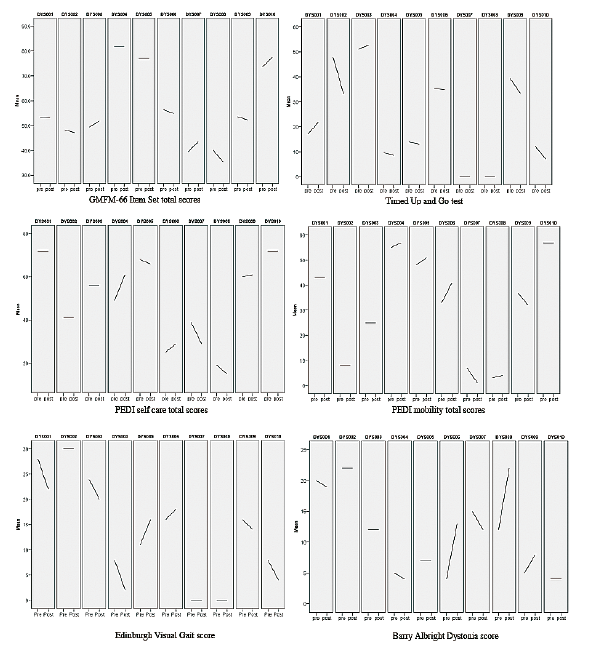 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize