


Jochen Schmitt1,2, Gottfried Wozel3, Marlene Garzarolli3, Antje Viehweg3, Michael Bauer4 and Karolina Leopold4
1Centre for Evidence-based Healthcare, Departments of 2Occupational and Social Medicine, 3Dermatology, and 4Psychiatry, Medical Faculty Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany
Psychiatric morbidity is frequent in patients with psoriasis. We compared the effectiveness of dermatological vs. interdisciplinary dermatological and psychiatric care for psoriasis. Adults with moderate-to-severe psoriasis were randomly allocated to dermatological (n = 24) or interdisciplinary care (n = 23) and treated accordingly. Primary endpoint was the mean change in Dermatology Life Quality Index (DLQI) at 6 months. Data was analysed by intention-to-treat. Mean ± SD change in DLQI was 7.5 ± 7.3 and 10.5 ± 9.9 after 6 months of dermatological and interdisciplinary care, respectively (p = 0.27). At baseline, 10 patients in the interdisciplinary treatment group (43%) had at least one psychiatric disorder. These patients showed significantly better DLQI response (DLQI change 14.8 ± 9.7) than patients receiving dermatological care only (p = 0.03). Ninety percent of psoriasis patients with DLQI scores exceeding psoriasis area and severity index (PASI) scores had comorbid psychiatric disease. Although psychiatric co-treatment is not generally required for patients with moderate-to-severe psoriasis, those patients with higher DLQI scores than PASI scores might benefit from interdisciplinary care. Key words: psoriasis; depression; quality of life; interdisciplinary care; clinical trial.
Accepted May 22, 2013; Epub ahead of print Aug 27, 2013
Acta Derm Venereol 2013; 93: xx–zz
Jochen Schmitt, MD, MPH, Centre for Evidence-based Healthcare, Medical Faculty Carl Gustav Carus, Technische Universität Dresden, Fetscherstraße 74, DE-01307 Dresden, Germany. E-mail: Jochen.Schmitt@uniklinikum-dresden.de
Psoriasis is a chronic systemic inflammatory disease that primarily affects the skin (1). The typical thickened, red, scaly plaques are often disfiguring and may cause substantial problems in everyday life (2). Health-related quality of life (HRQoL) describes the perceived influence of illness on everyday functioning, the achievement of life goals, and social and subjective feelings of well-being. The growing number of studies that include HRQoL as an outcome reflects the current broadening of the conceptualisation of psoriasis (3–5). Impaired HRQoL has been shown to be related with decreased work productivity and to be a major determinant of the high economic burden attributable to psoriasis (6).
Substantial proportions of patients with psoriasis suffer from comorbid mental disorders such as depression, anxiety, and suicidality (7–9). However, there is evidence that dermatologists often do not adequately detect psychiatric comorbidity (10–12). The lack of attention to psychiatric comorbidity may contribute to the dissatisfaction with psoriasis care in a substantial proportion of patients (13, 14).
Psoriasis-related HRQL impairment has been shown to predict depressive symptoms (15). Among psoriasis patients, depression and other psychiatric comorbidities appear undertreated, suggesting that integrated care models including dermatologists and mental health specialists might be most effective for at least a subgroup of psoriasis patients (16). Following the principles of evidence-based healthcare, the effectiveness of complex interventions and medical care models needs to be investigated by means of experimental, comparative research (17).
We conducted a pragmatic randomised controlled trial (RCT) to compare the effectiveness of dermatological vs. interdisciplinary dermatological and psychiatric care for adult patients with moderate-to-severe psoriasis. Our primary hypothesis was that interdisciplinary care by dermatologists and mental health specialists is not generally superior to dermatological care. We further hypothesised that a subgroup of psoriasis patients can be identified that benefits from interdisciplinary care. Based on our previous research (16) we speculated that patients with more severe psoriasis-related limitations in HRQoL might be at increased risk for psychiatric morbidity and might therefore benefit from interdisciplinary care.
Methods
Study type and participants
This pragmatic investigator-initiated RCT was conducted between November 2008 and June 2012 at the University Hospital Carl Gustav Carus Dresden, Germany. Patients aged 18 years or older with moderate-to-severe plaque psoriasis defined as PASI (18) ≥ 10 and significantly decreased HRQoL due to psoriasis defined as DLQI (19) score ≥ 10 were eligible. The only exclusion criteria were pregnancy and current suicidality. The majority of patients included in the trial had not been previously treated at our clinic and were recruited from the dermatological in-patient centre. The study was performed in accordance with the Declaration of Helsinki protocols. Ethical approval was given by the responsible institutional review board and all study subjects gave written informed consent before trial participation.
Interventions
Study participants were randomly allocated to receive dermatological care or interdisciplinary dermatological and psychiatric care for 6 months. In both groups, dermatological care was provided at the department of dermatology according to current treatment guidelines (20). All patients had at least 3 dermatological consultations, i.e. at baseline, after 3 months, and after 6 months. If required necessary by the dermatologist, additional visits were scheduled.
In patients randomly allocated to interdisciplinary care the participating psychiatrists conducted clinical examinations and diagnostic interviews in accordance to the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV criteria (21). In case of diagnosed mental disorder, psychiatric treatment was initiated in accordance with current clinical standards. All patients allocated to interdisciplinary care had at least two psychiatric assessments and consultations, i.e. at baseline and 6-month follow-up. If considered necessary by the psychiatrist, additional visits were scheduled.
Randomisation
During the baseline visit patients underwent central randomisation with the use of a permutated-block randomisation list (block length 6) with equal allocation to dermatological and interdisciplinary care. The allocation sequence was generated by Stata 8.0 for windows. Blinding was impossible as we compared models of care under real life conditions.
Study assessments and outcome measures
Age, sex, monthly household income, characteristics of psoriasis such as disease duration, presence/absence of psoriatic arthritis and nail involvement, as well as information on general and mental health status were assessed. At each study visit objective and subjective severity of psoriasis, previous, current, and newly prescribed anti-psoriatic treatment and patient satisfaction with psoriasis care were recorded. In patients allocated to interdisciplinary care, mental disorders were diagnosed using standardised clinical interviews based on the DSM-IV manual (21), and psychiatric treatments were recorded at both study visits.
The primary measure of effectiveness was the mean change in the DLQI (19) between baseline and 6-month follow-up. The DLQI consists of 10 questions considering the following domains: symptoms and feelings, daily activities, leisure, work and school, personal relationships, and the effects of treatment on daily life. The DLQI score ranges from 0 to 30 with higher scores reflecting worse psoriasis-related HRQL.
Secondary outcomes included the proportion of patients with ≥ 5 point improvement (i.e. minimum relevant improvement (22)) in DLQI, mean change in PASI, proportion of patients with PASI-75 and PASI-50 response, investigator’s global assessment of disease severity (IGA) on a 6-point Likert scale, and overall patient satisfaction with psoriasis care assessed on a 100 unit visual analogue scale with 0 reflecting total dissatisfaction and 100 reflecting maximal satisfaction. Patients were assessed by the same physicians at baseline and all following study visits.
Sample size calculation
In accordance with our primary hypothesis and primary study outcome sample size calculation was based on the two-group t-test of equivalence in means. The DLQI population equivalence limit was defined as 2.5 points, which is half of the minimum clinically relevant difference in DLQI for an individual patient (22). Assuming a common standard deviation in DLQI change in both groups of 3 points, calculations showed that 38 participants were needed for a study with 80% power and 5% significance level (nQuery Advisor). We aimed to recruit 46 patients to allow for a 20% dropout rate.
Statistical analysis
Proportions were compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were compared by the t-test.
To investigate the secondary hypothesis, patients from the interdisciplinary treatment group with and without a psychiatric diagnosis at baseline were differentiated for secondary analyses and compared to each other and to patients allocated to dermatological care with regard to patient characteristics, disease characteristics at baseline, and treatment response. Finally, separate univariate and multivariate regression models were fitted to (i) predict mental disorders prevalent at baseline and (ii) benefit from care in terms of DLQI-improvement.
Data analysis was by intention-to-treat, in which all randomised participants were included. Missing data were imputed by carrying forward the last known value. Data was analysed with Stata, version 11.0.
Results
Fig. 1 shows the Consort flowchart. From the 54 patients with psoriasis screened for eligibility, 47 were included in the study and randomly allocated to dermatological care (n = 24) or interdisciplinary care (n = 23). Forty-two participants (89%) completed the study per protocol (Fig. 1).
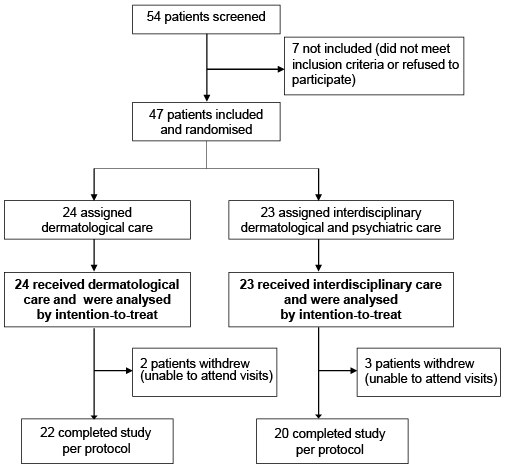
Fig. 1. CONSORT flowchart of trial profile.
Table I summarises socio-demographic and baseline characteristics of the 47 study participants that were randomised and analysed. Patients allocated to dermatological (n = 24) and interdisciplinary care (n = 23) did not differ significantly in any of these characteristics at baseline. Mean DLQI (19) and mean PASI (18) were 13.7 and 14.5 in the dermatological care group, and 17.4 and 16.0 in the interdisciplinary treatment group, respectively. The majority of patients (68%) had previously received conventional systemic treatment for psoriasis. Six patients in the dermatological care group and 2 patients in the interdisciplinary care group indicated that they had been ever diagnosed as having depression, and 2 patients in each treatment group received anti-depressive therapy at baseline (Table I).
Table I. Demographics and baseline characteristics of study participants
|
Treatment group |
||
|
Dermatological care (n = 24) |
Interdisciplinary care (n = 23) |
|
|
Age, years, mean ± SD |
49.5 ± 12.9) |
47.9 ± 18.4 |
|
Female sex, n (%) |
13 (54.2) |
13 (56.5) |
|
Monthly income (household), n (%) |
||
|
≤ 1,000 Euros 1,001–2,000 Euros 2,000–3,000 Euros > 3,000 Euros Missing information |
7 (29.2) 9 (37.5) 1 (4.2) 3 (12.5) 4 (16.7) |
6 (26.1) 10 (43.5) 5 (21.7) 1 (4.4) 1 (4.4) |
|
Characteristics of psoriasis Disease duration, years, mean ± SD Psoriatic arthritis, n (%) Nail involvement, n (%) Positive family history, n (%) |
28.3 ± 16.1 4 (16.7) 9 (37.5) 9 (37.5) |
26.4 ± 12.1 7 (30.4) 7 (30.4) 9 (39.1) |
|
Previous treatment of psoriasis Topical, n (%) UV/PUVA, n (%) Systemic non-biologic, n (%) Systemic biologic, n (%) |
24 (100) 18 (75.0) 17 (70.8) 10 (41.7) |
23 (100) 16 (69.6) 15 (65.2) 8 (34.8) |
|
DLQI, mean ± SD |
14.5 ± 6.8 [n = 22] |
17.4 ± 7.2 [n = 21] |
|
PASI, mean ± SD |
13.7 ± 7.4 |
16.0 ± 6.7 |
|
IGA, n (%) Mild Moderate Severe/very severe |
3 (12.5) 14 (58.3) 7 (29.2) |
0 (0) 16 (69.6) 7 (30.4) |
|
Patient satisfaction with psoriasis carea |
47.1 (28.8) [n = 21] |
46.4 (25.4) [n = 22] |
|
General morbidity Body mass index, mean ± SD Depressionb, n (%) Depressionc, n (%) Currently smoking, n (%) Alcohol consumptiond, n (%) |
29.3 ± 5.3 6 (25.0) 2 (8.3) 9 (37.5) 7 (29.2) |
27.4 ± 5.7 2 (8.7) 2 (8.7) 4 (17.4) 6 (26.1) |
aAssessed using a 100 unit visual analogue scale with 0 reflecting total dissatisfaction and 100 reflecting maximal satisfaction with treatment/medical care of atopic eczema. None of the observed differences between groups was statistically significant. bPreviously diagnosed by physician. cCurrently treated. d> 3 units/week.
DLQI: Dermatology life quality index; PASI: Psoriasis area and severity index; IGA: Investigator global assessment of disease severity.
Dermatological treatment did not differ between groups. At the end of study visit, 54% (n = 13) of patients in the dermatological treatment group received conventional systemic treatment, 21% (n = 5) received biological therapy. The corresponding proportions receiving conventional systemic and biological treatment in the interdisciplinary treatment group were 57% (n = 13) and 13% (n = 3), respectively.
Comparative effectiveness of dermatological vs. interdisciplinary care for moderate-to-severe psoriasis
From the 23 patients allocated to interdisciplinary care, 10 (43%) had at least one current mental disorder at baseline according to DSM-IV criteria. The diagnoses included affective disorders (major depressive disorder, n = 5; dysthymic disorder, n = 1; and depressive disorder NOS, n = 1), adjustment disorders (3 patients) and personality disorders (avoidant personality disorder: one patient and obsessive-compulsive personality disorder: one patient).
In 4 cases pharmacological psychiatric treatment was indicated because of the severity of depressive symptoms. From the patients receiving psychiatric treatment at baseline, 2 were diagnosed as having major depressive disorder, one patient as having depressive disorder NOS, and one patient as having dysthymic disorder. All patients received an anti-depressive medication (selective serotonin reuptake inhibitor and agomelatin). At the end of the study, 4 additional patients met criteria for current major depressive disorder and psychiatric treatment was recommended. All patients with a prevalent mental health disorder diagnosed in this study had depressive mood symptoms in the context of their diagnosis.
Table II summarises the results concerning the comparative effectiveness of dermatological vs. interdisciplinary care for psoriasis. In accordance with our primary hypothesis, interdisciplinary care was not superior to dermatological care for moderate-to-severe psoriasis at 6-months follow-up in terms of HRQoL response, or any other subjective of objective study outcome measure. Both regimens of care resulted in benefits concerning psoriasis-related HRQoL and clinical severity of psoriasis.
Table II. Comparative effectiveness of dermatological vs. interdisciplinary care for psoriasis (at 6 month visit)
|
Treatment group |
p-value |
|||
|
Dermatological care (n = 24) |
Interdisciplinary care (n = 23) |
|||
|
Primary outcome |
||||
|
Quality of life response Change in DLQI, mean ± SD |
7.5 ± 7.3 [n = 22] |
10.5 ± 9.9 [n = 21] |
0.27 |
|
|
Secondary outcomes |
||||
|
Quality of life response Proportion with reduction in DLQI ≥ 5 unitsa, n (%) |
14/21 (66.7) [n = 21] |
14/20 (70.0) [n = 20] |
0.82 |
|
|
Clinical response Change in PASI, mean ± SD PASI75 response, n (%) PASI50 response, n (%) |
8.0 ± 6.4 8/24 (33.3) 15/24 (62.5) |
7.1 ± 7.5 8/23 (34.8) 12/23 (52.2) |
0.63 0.92 0.47 |
|
|
Global disease severity IgA clear/almost clear, n (%) |
14/22 (63.6) |
10/20 (50.0) |
0.37 |
|
|
Patient satisfactionb, mean ± SD VAS-Score Change in VAS score since baseline |
61.1 ± 33.4 [n = 22] 12.3 ± 37.5 [n = 21] |
63.3 ± 32.1 [n = 22] 17.0 ± 35.9 [n = 22] |
0.83 0.68 |
|
aIn patients with baseline Dermatology Life Quality Index (DLQI) ≥ 5. bAssessed using a 100 unit visual analogue scale (VAS) with 0 reflecting total dissatisfaction and 100 reflecting maximal satisfaction with treatment/medical care of atopic eczema.
Characteristics and response of patients with and without mental disorder receiving interdisciplinary care
Table SI (available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1697) shows the characteristics of patients from the interdisciplinary treatment group stratified by presence (n = 10) or absence (n = 13) of mental disorder at baseline.
Psoriasis patients with mental disorder tended to be younger, to have a longer total duration of psoriasis, and were predominantly female. Psoriasis-related HRQoL decrease tended to be more pronounced in patients with mental health disorder (mean DLQI 19.9 vs. 15.8), whereas clinical severity of psoriasis tended to be less pronounced in patients with mental health disorder (mean PASI 12.6 vs. 18.6) (Table SII; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1697). Due to small numbers, none of these differences reached statistical significance. Dermatological treatment did not differ between patients with and without mental health disorder.
As detailed in Table SII, psoriasis patients with mental disorder benefited more from interdisciplinary care than patients without mental disorder in terms of HRQoL, but not in terms of clinical disease activity. The mean ± SD DLQI decrease was 14.8 ± 9.7 among patients with comorbid mental disorder, and 7.3 ± 9.1 in patients without mental disorder (p for between group difference = 0.08) (Table SII).
Compared with patients receiving dermatological care alone, patients from the interdisciplinary care group with comorbid mental disorder had a significantly better DLQI response (p = 0.03).
Predictors for comorbid mental disorder of patients with moderate-to-severe psoriasis
Further exploratory analysis indicated that 9 out of the 10 (90%) psoriasis patients from the interdisciplinary care group with comorbid mental disorder and 6/13 (46%) patients without comorbid mental disorder had a DLQI score greater than the PASI score (p = 0.03). Logistic regression analysis indicated an OR for comorbid mental health disorder of 10.5 (95% CI 1.02–108.58) for patients with DLQI > PASI compared to patients with DLQI ≤ PASI.
Predictors for decrease in DLQI after 6 months of treatment
The results of linear regression analyses on DLQI change from baseline to 6-month follow-up are presented in Table SIII (available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1697). In the multivariate model, interdisciplinary care for patients with comorbid mental disorder resulted in significantly better DLQI response (p = 0.005) than dermatological care, whereas interdisciplinary care for patients without mental disorder did not effect DLQI change compared to dermatological care (p = 0.50). Other variables significantly related to better DLQI response in the multivariate model were higher age (p = 0.044) and shorter duration of psoriasis (p = 0.002).
Discussion
Statement of principal findings
This study has 3 main findings relevant for clinical care of patients with moderate-to-severe psoriasis:
In accordance with our findings, previous studies documented that patients with chronic inflammatory skin disorders such as psoriasis (7, 8, 23, 24) or atopic dermatitis (25–28) are at increased risk for depression, anxiety, and other psychiatric disorders, and therefore may benefit from interdisciplinary care. Interestingly, psychiatric comorbidities in patients with psoriasis are independent from cardiovascular comorbidities, suggesting different etiological mechanisms (9).
Besides the hypothesis that the central effects of proinflammatory cytokines could play a causal role in depressive illness (29), psychosocial factors may induce increased comorbidity rates. Illness-related stress, feelings of stigmatisation and demoralisation due to psoriasis lesions, and dissatisfaction with treatment may contribute to the increased risk of depression in patients with psoriasis (15). Depression affects treatment adherence (30) and also modifies the perception of pruritus (31), a common symptom of psoriasis. The presented data indicate that depression and other mental disorders play a critical role in the life of many psoriasis patients. In the majority of the patients found to have a comorbid mental disorder in our study, diagnosis had not been made before in routine care. This indicates possible undertreatment of at least one subgroup of psoriasis patients.
It has been reported that clinical symptoms only account for a relatively small proportion of the total variability in emotional well-being in psoriasis (32). Interestingly, interdisciplinary treatment of comorbid psoriasis patients resulted in improved dermatology specific HRQoL. Comorbid mental disorder might at least partially account for the frequently observed mismatch of objective and subjective severity of psoriasis, i.e. high HRQoL limitations despite relatively low intensity and extent of clinical signs of psoriasis (15, 16, 33).
In our study, shorter total duration of psoriasis was independently associated with a higher likelihood of DLQI response after 6 months of treatment. Psoriasis patients with prevalent mental disorder tended to be younger and to have longer disease duration than patients without comorbid mental disorder. It may be speculated, that specific psoriasis-related problems in everyday life lead to more general limitations in QoL with chronification of psoriasis over time and may finally increase the susceptibility for a mental disorder. This is not a phenomenon specific to psoriasis, but a potential result from any chronic somatic disease. Between 20 and 25% of people with chronic medical conditions will become depressed during the course of their disease (34).
Strengths and weaknesses of the study
Strengths of our study include random allocation of consecutive psoriasis patients to dermatological or interdisciplinary care. To allow generalisability to routine care we did not standardise dermatological care or psychiatric care. One important caveat is, however, that we recruited mainly from the dermatological in-patient center. We chose that approach because we aimed to include patients with a current exacerbation of psoriasis and/or clear indication to optimise dermatological care. Dermatological in-patient treatment is quite common in Germany, and psoriasis is among the most frequent dermatological diagnoses for hospitalisation (35). Due to the fact that psychiatric examination including a diagnostic interview according to DSM-IV does not only allow diagnoses, but also has therapeutic effects, we decided not to explore the mental health status of psoriasis patients allocated to dermatological care. Interdisciplinary care was also beneficial in those comorbid patients who did not receive specific psychiatric therapy. Sociodemographic characteristics and characteristics of psoriasis did not differ between study groups, and randomisation most likely ensured a balance of study groups in terms of possible other confounders, so that we believe our results to be internally valid.
Implications for clinicians and policymakers
Concurrent mental disorder affects HRQoL of patients with moderate-to-severe psoriasis at least as much as the clinical severity of their psoriatic lesions. Patients with psoriasis, in whom the DLQI score is higher than the PASI score, have a high likelihood for prevalent comorbid mental disorder. Dermatologists treating patients with psoriasis should therefore closely collaborate with mental health specialists and consider referral of psoriasis patients fulfilling the above described combination of subjective and objective severity of psoriasis.
ACKNOWLEDGEMENTS
Funding: This was an investigator-initiated trial partly sponsored by Wyeth. The trial was planned, conducted, analysed, and reported independently by the authors.
Competing interest: JS served as a consultant for Novartis and Abbott. GW served as a consultant for Pfizer and received research funding from Pfizer. MG has received speaker honoraria from BMS. AV has received speaker honoraria from Abbott, Janssen Cilag and Pfizer. MB has received Grant/Research Support from The Stanley Medical Research Institute and NARSAD. He is a consultant for AstraZeneca, Lilly, Servier, Janssen-Cilag, Lundbeck and BMS & Otsuka. Dr. Bauer has received speaker honoraria from AstraZeneca, Lilly, GlaxoSmith Kline, Lundbeck, BMS, Otsuka and Pfizer.
KL has received speaker honoraria from AstraZeneca, BMS, Pfizer, Janssen-Cilag, Lundbeck and Lilly.
REFERENCES


