


Michaela E. R. Kopyciok1, Hartmut F. Ständer2,3, Nani Osada4, Sabine Steinke1 and Sonja Ständer1
1Center for Chronic Pruritus and Department of Dermatology, 4Department of Medical Informatics and Biomathematics, University Hospital Münster, Münster, 2Dermatological Practice, Bad Bentheim, 3Department of Dermatology, Klinikum Dortmund gGmbH, Dortmund, Germany
Pruritus is a frequent sensation in dermatoses, but its prevalence in patients in dermatological practices has not been fully studied. The aim of this cross-sectional study is to investigate its prevalence and characteristics in all patients attending a dermatology practice in Germany over a period of one week (n = 334; 52.7% female; median age 45.0 years). The point prevalence of pruritus in this study population was 36.2% (87.6% of whom had chronic pruritus). It inhibited the everyday life of 73.6% of all patients, with 77.7% reporting a frequently to permanently experienced moderate intensity. (5.2 ± 2.3 on the numerical rating scale). Of the patients, 52.1% had previously consulted their general practitioner, and 62% had visited the dermatologist due to pruritus. This study shows that pruritus is a highly prevalent, clinically and economically relevant symptom in dermatological practices. The majority of patients suffering from chronic pruritus are severely burdened and medically underserved. Dermatologists should be aware that pruritus also occurs frequently in patients who do not primarily present due to their symptoms. Key words: pruritus; itch; prevalence; dermatological practice.
Accepted Jun 8, 2015; Epub ahead of print Jun 12, 2015
Acta Derm Venereol 2015; XX: XX–XX.
Sonja Ständer, Center for Chronic Pruritus and Department of Dermatology, University Hospital Münster; Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: sonja.staender@uni-muenster.de
Although pruritus is frequent among the general population and dermatological patients, there have been few studies on its prevalence in primary care facilities and dermatological practices. Furthermore, epidemiological studies on pruritus in the general population are rare and difficult to compare due to different study designs and the lack of standardized measures (1). The largest study, to date conducted in the general population of Norway, revealed a prevalence of 8%. However, this study did not differentiate between acute (AP) and chronic pruritus (CP, defined as pruritus lasting 6 weeks and longer [2, 3]) and was also limited by the fact that it was conducted in a single city. More recent studies analysing the prevalence of CP in Germany have revealed an even higher prevalence than expected and showed a point prevalence of 13.5% in the general population (4) and 16.8% in working adults (5).
The German healthcare system provides 2 general opportunities for referral to a specialist. The patient can either directly self-refer to a dermatologist or general practitioner (GP), or their GP will refer them to a dermatologist. These dermatological practices represent an important contact point for patients with pruritus before being referred to specialized itch clinics. Thus, information about the features of pruritus, as well as the distribution of AP and CP in these patients, is important for clinicians and researchers. However, this information has not been investigated in representative studies so far.
The aim of this cross-sectional study was to investigate the prevalence and characteristics of pruritus, as well as the related disease burden and healthcare situation, in a large dermatological population attending a dermatology practice.
PATIENTS AND METHODS
Subjects and study design
A random cohort of patients attending a general dermatology practice (no specialization, no pre-visit selection of patients; 3 dermatologists working in the practice) in a rural area in north-western Germany (Bad Bentheim, Lower Saxony) was included. All patients attending this practice within a period of one week (February 28 to March 4, 2011), independent of the reason for their consultation, were asked to complete a one page questionnaire regarding their current symptoms (Fig. S11). The patients’ questionnaire was developed based on the modified German Itch Questionnaire (6) and is comprised of 11 questions about the current presence of pruritus (yes or no), its duration (< 6 weeks for acute itch or > 6 weeks for chronic itch [2]), localization (10 regions of the body to choose from) and daily frequency (seldom [1] to permanent [4]). Pruritus intensity on the day of examination was measured using a numerical rating scale (NRS) ranging from 0 to 10 (7). In addition, the questionnaire addresses quality of life aspects by asking for the impact of pruritus on sleep, emotional burden and impairment of daily life on a scale from 0 (none) to 3 (severe). Patients were further asked if they had consulted a GP before because of pruritus (yes or no), whether pruritus was their reason for visiting the dermatology practice and which forms of pretreatment had been used (oral/topic prescribed or over-the-counter [OTC] medication). Current dermatological diagnoses of each patient were assessed by the dermatologists working in the practice. Written consent was obtained from all patients and the study was approved by the local ethics committee (number 2007-413-f-S).
Statistical analysis
Data was assembled with Microsoft Excel (Version 2010, Microsoft®, Redmond, WA, USA) and statistical analysis carried out using IBM-SPSS® Statistics software for Microsoft® Windows Version 18.0 (July 2009, SPSS Inc., Chicago, IL, USA). Categorical variables are expressed as frequencies and percentages, whereas continuous variables are presented as means ± standard deviations (SD) or median and interquartile ranges (IQR). Before statistical testing, the Kolmogorov-Smirnov test was used to analyse each continuous variable for normal distribution. For normally distributed samples, the parametric t-test for independent samples (2-sided) was used to analyse the differences in continuous variables between 2 study groups. For not normally distributed samples, the non-parametric Mann-Whitney U test (2 samples) and Kruskal-Wallis test (> 2 samples) were used. Post hoc comparison with Dunn’s procedure was applied to determine the differences between 3 diagnosis groups. Depending on the sample size, the χ2 test or Fisher’s exact test was used to compare the distributions of study groups. A p-value < 0.05 was considered statistically significant in all analyses.
RESULTS
Cohort description and demographic data
A total of 382 patients attended the practice within the evaluated period (Fig. 1). Forty-eight refused to participate and were not included in the study (no demographic or clinical information was obtained from these patients). A total of 334 patients (mean age, 43.7 ± 21.8 years; median 45 years; 158 males [47.3%], 176 females [52.7%]), participated in the study (participation rate 87.4%) (Table I).
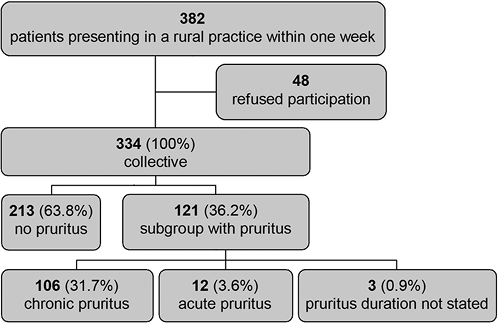
Fig. 1. More than one-third of patients at a dermatological practice had pruritus. Percentages are provided in relation to the participating patients (n = 334).
Table I. Demographic data and characteristics of patients with pruritus
|
Collective (n = 334) |
Subgroup with pruritus |
||||
|
Total (n = 121) |
Acute (n = 12) |
Chronic (n = 106) |
Durationa (n = 3) |
||
|
Age, years |
|
|
|
|
|
|
Mean ± SD |
43.7 ± 21.8 |
45.0 ± 21.4 |
34.3 ± 24.5 |
46.0 ± 20.5 |
51.3 ± 35.1 |
|
Median |
45.0 |
46.0 |
29.0 |
48.5 |
68.0 |
|
Sex, n (%) |
|||||
|
Male |
158 (47.3) |
52 (43.0) |
3 (25.0) |
47 (44.3) |
2 (66.7) |
|
Female |
176 (52.7) |
69 (57.0) |
9 (75.0) |
59 (55.7) |
1 (33.3) |
|
Frequency of symptoms, n (%) |
|||||
|
Permanent |
8 (2.4) |
8 (6.6) |
0 |
7 (6.6) |
1 (33.3) |
|
Almost Permanent |
19 (5.7) |
19 (15.7) |
2 (16.7) |
17 (16.0) |
0 |
|
Frequent |
67 (20.1) |
67 (55.4) |
7 (58.3) |
58 (54.7) |
2 (66.7) |
|
Seldom |
25 (7.5) |
25 (20.7) |
3 (25.0) |
22 (20.8) |
0 |
|
Not answered |
2 (0.6) |
2 (1.7) |
0 |
2 (1.9) |
0 |
|
Pruritus intensity, n (%) |
|||||
|
Mean ± SD |
n.d. |
5.2 ± 2.3 |
4.0 ± 2.0 |
5.3 ± 2.3 |
6.3 ± 2.3 |
|
Median (range) |
5.0 (1–10) |
3.0 (1–8) |
5.0 (1–10) |
5.0 (5–9) |
|
|
Localization, n (%) |
|||||
|
Face |
34 (10.2) |
34 (28.1) |
0 |
33 (31.1)* |
1 (33.3) |
|
Neck |
22 (6.6) |
22 (18.2) |
2 (16.7) |
20 (18.9) |
0 |
|
Back |
42 (12.6) |
42 (34.7) |
5 (41.7) |
35 (33.0) |
2 (66.7) |
|
Breast/stomach |
24 (7.2) |
24 (19.8) |
2 (16.7) |
22 (20.8) |
0 |
|
Anogenital |
17 (5.1) |
17 (14.1) |
0 |
17 (16.0) |
0 |
|
Head |
44 (13.2) |
44 (36.4) |
4 (33.3) |
37 (34.9) |
3 (100) |
|
Arm |
54 (16.2) |
54 (44.6) |
7 (58.3) |
45 (42.5) |
2 (66.7) |
|
Hand |
35 (10.5) |
35 (28.9) |
3 (25.0) |
32 (30.2) |
0 |
|
Leg |
69 (20.7) |
69 (57.0) |
7 (58.3) |
60 (56.6) |
2 (66.7) |
|
Feet |
35 (10.5) |
35 (28.9) |
1 (8.3) |
33 (31.1) |
1 (33.3) |
|
Quality of life, n (%) |
|||||
|
Emotional burden, n (%) |
|||||
|
Severe |
11 (3.3) |
11 (9.1) |
1 (8.3) |
10 (9.4) |
0 |
|
Moderate |
52 (15.6) |
52 (43.0) |
3 (25.0) |
49 (46.2) |
0 |
|
Low |
44 (13.2) |
44 (36.4) |
5 (41.7) |
37 (34.9) |
2 (66.7) |
|
None |
13 (3.9) |
13 (10.7) |
3 (25.0) |
9 (8.5) |
1 (33.3) |
|
Not answered |
1 (0.3) |
1 (0.8) |
0 |
1 (0.9) |
0 |
|
Sleeplessness, n (%) |
|||||
|
Severe |
8 (2.4) |
8 (6.6) |
0 |
8 (7.5) |
0 |
|
Moderate |
25 (7.5) |
25 (20.7) |
2 (16.7) |
22 (20.8) |
1 (33.3) |
|
Low |
47 (14.1) |
47 (38.8) |
4 (33.3) |
43 (40.6) |
0 |
|
None |
41 (12.3) |
41 (33.9) |
6 (50.0) |
33 (31.1) |
2 (66.7) |
|
Not answered |
0 |
0 |
0 |
0 |
0 |
|
Restriction in daily life, n (%) |
|||||
|
Severe |
6 (1.8) |
6 (5.0) |
0 |
6 (5.7) |
0 |
|
Moderate |
33 (9.9) |
33 (27.3) |
3 (25.0) |
30 (28.3) |
0 |
|
Low |
50 (15.0) |
50 (41.3) |
3 (25.0) |
46 (43.4) |
1 (33.3) |
|
None |
30 (9.0) |
30 (24.8) |
5 (41.7) |
24 (22.6) |
1 (33.3) |
|
Not answered |
2 (0.6) |
2 (1.7) |
1 (8.3) |
0 |
1 (33.3) |
anot determined; *chronic pruritus is significant vs. acute pruritus (p = 0.019).
Prevalence and duration of pruritus
The point prevalence of pruritus in all patients included in the study (n = 334) was 36.2% (n = 121, 95% confidence interval [95% CI] 0.31–0.41) (Fig. 1) with no significant difference between men (32.9%, 95% CI 0.34–0.52) and women (39.2%, 95% CI 0.48–0.66) (p = 0.232). According to the International Forum for the Study of Itch (IFSI), CP was defined as pruritus of at least 6 weeks’ duration (2). We found that 87.6% of all patients with pruritus (n = 121) had CP (n = 106) upon presentation, whereas only 9.9% (n = 12) had AP; 2.5% (mostly elderly patients with a median age of 68 years) did not specify the duration of their pruritus. Referring to the total study collective, this is a point prevalence of 31.7% for CP (95% CI 0.27–0.37) and 3.6% for AP (95% CI 0.02–0.06). Regarding age distribution, patients with CP were, on a mean average, 11.7 years older than patients with AP (CP: 46.0 ± 20.5 years; AP: 34.3 ± 24.5 years; p = 0.068). Men with pruritus were, on average, 8.3 years older than the women (men 49.7 ± 20.9 years; women 41.4 ± 21.2 years; p = 0.033) (Fig. 2). No further significant difference between the sexes was evident in either the whole study population or within the subgroups with pruritus.
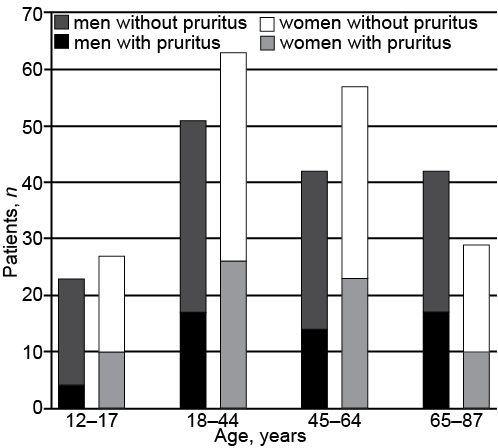
Fig. 2. Sex and age distribution in the collective. More than one-third (36.2%; n = 121) of patients in the collective (n = 334) had pruritus. The age distribution of the subgroup with pruritus (mean ± SD 45.0 ± 21.4 years) does not differ from that of the whole collective (mean ± SD 43.7 ± 21.8 years). Men with pruritus were, on a mean of 8.3 years older than women (p = 0.033).
Dermatological diagnoses
Current diagnoses, as defined by dermatologists, were mainly inflammatory dermatoses (e.g. atopic dermatitis [AD], eczema [e.g. xerotic eczema, seborrhoeic eczema, dyshidrotic eczema, hand eczema, nummular eczema], psoriasis vulgaris, acne vulgaris), but also multiple benign (e.g. seborrhoeic keratosis) and malignant (e.g. actinic keratosis, basal cell carcinoma) neoplasms. In the majority of cases, the clinical diagnoses were made according to consented dermatological criteria (e.g. criteria of Hanifin & Rajika for AD [8]), and in a minority of patients, confirmed histologically. No cases of urticaria were found. In case of drug reactions, we noted drug allergies, allergic contact dermatitis and drug intolerances; wasp venom allergy was recognized in one outlying case. Patients could be given more than one dermatological diagnosis. The total number of diagnoses per patient did not differ significantly between patients with and without pruritus (1.3 and 1.2 diagnoses per patient, respectively). Three patient groups were primarily affected by pruritus: AD (83.3%, of whom 96% with CP), other forms of eczema (56.5%, of whom 84.6% with CP) and psoriasis vulgaris (48.6%, of whom 88.2% with CP). However, only in the groups with AD and other forms of eczema, the number of patients with pruritus was greater than those without pruritus (p < 0.001 and p = 0.002, respectively; odds ratio 10.83 [95% CI 4.0–29.2] for AD and 2.64 [95% CI 1.4–5.0] for other forms of eczema) (Table II). All other diagnoses showed a similar percentage among patients with and without pruritus, or were significantly more frequent in patients without pruritus, as noted for neoplasms (p = 0.005) (Table II). There was no difference in the distribution of diagnoses between patients with AP and CP. When looking at sex difference in the subgroup with pruritus, only psoriasis vulgaris showed a tendency to be more frequent in males (p = 0.051).
Table II. Correlation between pruritus and related diagnoses
|
Diagnosis |
Study population (n = 343) n (%) |
Subgroup with pruritus |
||||
|
Total (n = 121) n (%) |
Diagnosis, % n (%) |
Acute (n = 12) n (%) |
Chronic (n = 106) n (%) |
Duration n.d. (n = 3) n (%) |
||
|
Atopic dermatitis |
30 (9.0) |
25 (20.7) |
25/30 (83.3)*** |
1 (8.3) |
24 (22.6) |
0 (0.0) |
|
Eczemaa |
46 (13.8) |
26 (21.5) |
26/46 (56.5)** |
3 (25.0) |
22 (20.8) |
1 (25.0) |
|
Psoriasis |
35 (10.5) |
17 (14.1) |
17/35 (48.6) |
1 (8.3) |
15 (14.2) |
1 (25.0) |
|
Venous diseaseb |
37 (11.1) |
12 (9.9) |
12/37 (32.4) |
2 (16.7) |
10 (9.4) |
0 (0.0) |
|
Neoplasm |
88 (26.3) |
21 (17.4) |
21/88 (23.9)** |
2 (16.7) |
18 (17.0) |
1 (25.0) |
|
Acne, rosacea |
53 (15.9) |
14 (11.6) |
14/53 (26.4) |
2 (16.7) |
12 (11.3) |
0 (0.0) |
|
Infestation |
50 (15.0) |
17 (14.1) |
17/50 (34.0) |
2 (16.7) |
14 (13.2) |
1 (25.0) |
|
Allergy |
20 (6.0) |
7 (5.8) |
7/20 (35.0) |
1 (8.3) |
6 (5.7) |
0 (0.0) |
|
Various |
47 (14.1) |
16 (13.2) |
16/47 (34.0) |
1 (8.3) |
15 (14.2) |
0 (0.0) |
Multiple diagnoses were possible for one patient: acomprises e.g. xerotic eczema, seborrhoeic eczema, dyshidrotic eczema, hand eczema, nummular eczema; bcomprises chronic venous insufficiency, varicosis, thrombophlebitis, venous ulcers, post-thrombotic ulcers, post-thrombotic syndrome, spider veins, stasis oedema, stasis dermatitis; n.d.: not determined. ***Atopic dermatitis is significantly associated with pruritus (p < 0.001; OR=10.83; 95% CI 4.0–29.2); **eczema is significantly associated with pruritus (p = 0.002; OR = 2.64; 95% CI 1.4–5.0); **neoplasm is significantly not associated with pruritus (p=0.005; OR = 0.46; 95% CI 0.26–0.80).
Characteristics of pruritus and effects on quality of life aspects
Concerning the daily frequency of pruritus, 77.7% of patients had pruritus frequently to permanently (Table I) without a significant difference in AP and CP. The intensity of pruritus on the day of examination had a median of 5.0 (IQR 1–10) NRS points (Fig. S21). There was no significant difference in pruritus intensity between AD, other forms of eczema and psoriasis vulgaris (Fig. S21). Patients with CP (median 5.0, IQR 1–10) reported a 2.0 NRS points higher intensity of pruritus than patients with AP (median 3.0, IQR 1–8) (p = 0.072). Most patients with pruritus (AP 58.3%; CP 56.6%) reported having symptoms on their lower extremities (Table I).
Pruritus had a negative effect on the daily life of 73.6% (n = 89) of all patients (n = 121, 36.2% of all patients), and 32.3% (n = 39) described this impairment as moderate or severe (Table I). Sleeplessness due to pruritus was reported by 66.1% of the patients, with 27.3% describing this to be of at least moderate intensity. Pruritus-related emotional burden was observed in 88.4% of patients; 52.1% described this burden to be moderate to severe. There were no differences in any of these parameters between AP and CP, or between men and women. The impact on quality of life (QoL) aspects was further investigated for pruritus patients with AD, other forms of eczema and psoriasis vulgaris. All 3 diagnoses were associated with a severe restriction of daily life (AD 88.0%; other forms of eczema 76.9%; psoriasis 88.2%) and sleeplessness (AD 72.0%; other forms of eczema 80.8%; psoriasis 76.5%); there were no significant differences between the 3 groups. Almost all of the patients diagnosed with these diseases (AD 100.0%; other forms of eczema 92.3%; psoriasis 100%) experienced emotional burden.
Aspects of healthcare
Among the subgroup of patients with pruritus, 52.1% reported that they had consulted their GP due to pruritus before being referred to the dermatologist. Prior GP consultation rate was higher for CP (58.5%) than for AP (8.3%), with no difference between dermatoses and sex (Table SI1). Sixty-two percent of the patients with pruritus stated that they were consulting their dermatologist because of itch. This percentage was similar for CP (64.2%) and AP (50.0%) (p = 0.475) (Table SI1). Patients attending due to pruritus had significantly higher NRS scores (5.7 ± 2.5; p = 0.005) and had AD (30.7%; p = 0.001) or other forms of eczema (28.0%; p = 0.039) significantly more often than patients attending for another reason (NRS, 4.4 ± 1.6; AD: 4.7%; other forms of eczema: 11.6%). Pretreatment was significantly more frequent for CP (82.1%) than for AP (50.0%) (p = 0.01), with no significant differences among the different forms of therapy (Table SI1). The highest number of pretreatments was seen in the group of patients with AD (76.7%), followed by other forms of eczema (45.7%) and patients with psoriasis vulgaris (42.9%) (Table SI1). QoL was significantly more impaired in patients with pretreatment than in patients without (impairment of daily life: p = 0.009; emotional burden: p = 0.01; sleeplessness: p = 0.03). Also, the pruritus intensity measured with NRS was higher in patients with pretreatment (median 5, IQR 4–7) than without (median 4, IQR 3–5) (p = 0.001).
DISCUSSION
To the best of our knowledge, this cross-sectional study is the first to evaluate the prevalence of pruritus and its characteristics, associated disease burden and the underlying healthcare situation in a cohort of dermatology practice patients. We noted a high pruritus point prevalence of 36.2%. Only one study, a national sample of the French population, showed a similar high prevalence (29.8%) (9), while other studies revealed lower numbers (8–17%) (3, 5, 10). However, the French study was not conducted in patients attending a dermatology practice and did not distinguish between AP and CP (9). Most importantly, most patients of our cohort had CP (31.7%), while only 3.6% had AP. CP is defined by a longer duration of itch (6 weeks and longer [2]) compared with AP (up to 6 weeks’ duration). As expected (1), patients with chronic relapsing dermatoses such as atopic dermatitis, various forms of eczema (e.g. xerotic eczema, dyshidrotic eczema, nummular eczema) and psoriasis vulgaris were found to be highly affected by pruritus (11). These diagnoses also had a high rate of CP and a high number of pretreatments. Usually, dermatological therapies, both topical and systemic, lead to resolution of inflammation in AD, eczema and psoriasis vulgaris along with the cessation of pruritus. However, up to 77% of our patients had used some form of pretreatment related to their pruritus without improvement. They still had pruritus frequently to permanently (78%), in moderate to severe intensity, and consequently, experienced impairment in their daily life (74%). This reflects, on one hand, that patients with severely itchy dermatoses exhibit a high economic need, as they had several OTC and prescribed pretreatments, yet still required treatment. On the other hand, it suggests that the applied antipruritic therapies were not potent enough (only 12% of patients received systemic therapy). This observation, particularly in the context of the high burden of these patients, points to a weakness in the current quality of medical care for patients with pruritus, an issue that needs to be urgently addressed. This is a well-known clinical problem for several reasons: the lack of availability and use (especially by non-pruritus experts) of novel and potent antipruritic therapies and the lack of area-wide specialized itch centers (12); the use of weak or non-effective therapies, such as OTC drugs taken either as self-medication or applied by caregivers (as physicians may tend to underestimate the severity and resistance of pruritus), promotes the maintenance of the symptoms. However, the failure to show improvement might also be due to a lack of patient compliance. To overcome this gap in medical care, several issues should be addressed in the future. As a rapid and potent therapy is usually advised in patients with pruritus in order to avoid progression to CP (13), it is recommended that caregivers follow the CP Guideline which was published in 2012 (13). Furthermore, a more intensive involvement and communication with insurance companies, who cover the costs for treatment, would be preferable in order to discuss the modalities of offering improved and structured medical care to patients. Finally, establishment of more specialized itch centres could improve the medical care of patients with pruritus.
Besides the high frequency of pruritus in dermatological patients, our data indicates that the most severely and continuously affected patients go to a specialized dermatologist more frequently than other more weakly affected patients. The percentage of prior GP consultation and the percentage of patients stating that pruritus was the reason for the current visit to the dermatologist practice were significantly higher in pretreated patients with CP than with AP. It seems likely that moderately affected patients are self-treated or only visit their GP, yet there are no current studies investigating the prevalence and severity of pruritus in general practice.
In our study, 38% of the patients affected by pruritus did not visit the dermatologist because of their itch but due to various reasons, although they are severely affected. This dichotomy might be explained by the fact that a lot of patients are initially insufficiently treated and thus might believe that their pruritus cannot be effectively controlled. This is further supported by our findings: few patients are treated with systemic antipruritic drugs, and a low percentage of patients visit a specialist.
In our study, men and women were almost equally affected by pruritus, but the men were significantly (8.3 years) older than the women. This is in line with our previous analysis demonstrating that men with CP were significantly older (3 years) than women (14). General socioeconomic studies report that men seek medical advice later and less frequently than women (15, 16). However, these studies do not specialize in pruritus. Although recent evidence point out that the duration of pruritus in men and women is similar (14), the sex difference seen in our study is probably not due to a delay in male patients seeking medical advice. Our data rather supports the assumption that, despite being equally affected by pruritus, men show a delay in the development of itch. Further research is necessary into this aspect in epidemiological studies of patients with CP. It is well-known that the most impacted group of patients with CP is the elderly (17, 18). With increasing age, there is also an increase in diseases and other comorbidities associated with pruritus (19). This is underlined by the age distribution in our study indicating that patients reporting CP were, on average, 11.7 years older than patients with AP. Interestingly, despite higher age, higher itch intensity and pronounced localization of CP in the facial region, AP and CP did not differ in characteristics such as frequency of occurrence within a period of 24 h, and impairment of QoL aspects. This data determines that there is a similar severity of AP and CP.
Pruritus, especially CP, is well-known for having a severely negative impact on a patient’s QoL (20–22). We utilized several questions on important aspects of QoL instead of elaborated QoL scores, such as DLQI (23) and ItchyQol (24), as these are rather complex and long. Emotional burden was the major factor affecting QoL in our patients (88%), followed by sleeplessness (66.1%). The crucial role of emotional burden in patients with CP was also emphasized by a French study showing that 42% of patients with CP declared the symptoms as burdensome (25). Furthermore, a recent European study in dermatological outpatients proved the large impact of skin diseases mostly associated with pruritus on DLQI, depression rate and anxiety (26, 27). Zachariae et al. (28) also demonstrated that sleeplessness might be a relevant factor influencing QoL, as it may be a link between pruritus and depression. These results underline the impact of pruritus on patients’ QoL. Patients with pruritus should therefore always be questioned and examined for psychological impairment.
In conclusion, our study shows a high point prevalence of pruritus in dermatological practice patients and thus underlines its major medical and economic importance. We furthermore demonstrate that the vast majority of patients with pruritus have CP. However, there are several limitations to our study. Climatic factors have to be taken into account when regarding the prevalence of pruritus. Another limitation to our study arose from its design. Our aim was to describe the point-prevalence of pruritus in a dermatology practice. We used a physician-based assessment of current dermatological diseases, which did not assess comorbdity, alongside a patient-based questionnaire on pruritus. Thus, the presence of non-dermatological medical causes of pruritus cannot be excluded. Our study is the first to demonstrate the need for recognition of pruritus in dermatological practice patients, as pruritus is frequent, and patients remain medically underserved and highly burdened.
ACKNOWLEDGEMENTS
The authors would like to thank Rajam Csordas-Iyer and Emily Burnett for assistance in manuscript preparation, Merle Pilz for data assessment in the practice, and Drs Markward Ständer and Joas Hofsommer for participating in the study group.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2166
REFERENCES


