


1School of Medicine, University of Tampere, 2Department of Internal Medicine, Tampere University Hospital, 3Tampere Center for Child Health Research, University of Tampere and Tampere University Hospital, 4Department of Gastroenterology and Alimentary Tract Surgery, 5Department of Dermatology, Tampere University Hospital, 6Tampere School of Health Sciences, University of Tampere, and 7Finnish Coeliac Society, Tampere, Finland
Dermatitis herpetiformis (DH) is an extraintestinal manifestation of coeliac disease. The burden of illness in untreated coeliac disease is known to be considerable, but corresponding evidence for DH is lacking. In this study the burden of DH was evaluated prospectively in 52 patients newly diagnosed with DH using a study questionnaire and a validated Psychological General Well-Being (PGWB) questionnaire. The PGWB scores were compared with those of 110 healthy controls. Quality of life was significantly (p < 0.001) lower among patients with DH at the time of diagnosis, but after one year on a gluten-free diet their quality of life was at same level as that of the controls. The presence of gastrointestinal symptoms was shown to significantly increase the burden of untreated DH. We conclude that there is a significant burden related to untreated, but not to treated, DH, and the burden is even greater among DH patients with gastrointestinal symptoms.
Key words: dermatitis herpetiformis; burden of illness; quality of life; gastrointestinal symptoms; coeliac disease; gluten-free diet.
Accepted May 23, 2016; Epub ahead of print May 31, 2016
Acta Derm Venereol 2017; 97: 58–62.
Corr: Teea Salmi, Department of Dermatology, Tampere University Hospital, PO Box 2000, FIN-33521 Tampere, Finland. E-mail: teea.salmi@uta.fi
Dermatitis herpetiformis (DH) is an extraintestinal manifestation of coeliac disease. The predominant symptom in DH is an itching blistering rash, which is triggered by ingestion of gluten (1). Diagnosis of DH is based on typical cutaneous symptoms and demonstration of granular immunoglobulin A (IgA) deposits in a skin biopsy (2). In addition to the skin manifestations, patients with DH also evince a coeliac-type gluten-sensitive small-bowel enteropathy, the majority having some degree of small-bowel mucosal villous atrophy (3). However, according to the present understanding, DH patients rarely experience gastrointestinal (GI) symptoms, although the evidence is scant. DH and coeliac disease also share the same immunogenic background, as both groups of patients have circulating immunoglobulin A (IgA) antibodies against endomysium (EmA) and tissue transglutaminase (TG2) auto-antigens. There is also a similar genetic background between the 2 diseases, with a strong association with human leukocyte antigen (HLA)-DQ2, and the disorders often occur in families (1). Consistently with coeliac disease, the treatment of choice in DH is a life-long gluten-free diet (GFD), which ameliorates both the rash and the small-bowel mucosal changes (4).
The disease burden is known to be considerable in coeliac disease; the diagnostic delay is frequently long, resulting in a burden of ongoing symptoms, a decrease in quality of life, increased use of on-demand medication, and the economic burden of healthcare utilization for society (5–7). Most patients with coeliac disease benefit from a GFD; their well-being increases and symptoms are alleviated (6, 8). However, dieting is troublesome and compliance difficult (9, 10). A substantial burden of illness is also related to a number of itching chronic skin diseases, such as psoriasis and atopic dermatitis (11, 12). Although DH is an itching chronic skin disease and an extraintestinal manifestation of coeliac disease, knowledge of its detriments is scarce. The aim of this prospective study was to assess the burden of illness during the year prior to DH diagnosis and one year after initiation of GFD treatment, and to determine whether GI complaints contribute to the burden of DH.
The data used in this study were obtained from a nationwide cohort of patients newly diagnosed with coeliac disease. Information was gathered in collaboration with the Finnish Coeliac Society, which currently has over 20,000 members. In Finland, approximately 70% of all patients with coeliac disease join the Finnish Coeliac Society shortly after being diagnosed. Between February 2007 and May 2008, a study questionnaire (see below in detail) was posted to all new members of the Finnish Coeliac Society. From among the respondents, patients over 16 years of age with skin biopsy-proven DH were enrolled as study patients. A follow-up questionnaire was sent to all respondents after one year. At follow-up, a telephone reminder was given to all non-respondents. For the present purpose, the DH patients were divided into 2 groups based on the presence or absence of self-reported GI symptoms at the time of diagnosis.
The control group comprised 110 adults who considered themselves healthy and had no first-degree relatives with coeliac disease. They were recruited from the close neighbourhood and from among friends of the patients with coeliac disease, the aim being to obtain a control group from a social and residential environment similar to that of the study patients.
The study protocol was approved by the review board of the Finnish Coeliac Society in compliance with all applicable Finnish laws for registered organizations, and covering the protection of human suspects. Informed consent was obtained from all study subjects after a full written explanation of the aims of the study, including considerations regarding ethics, data protection and the anonymous deposition of the questionnaires. Furthermore, all control patients gave their written informed consent and the study protocol involving the control patients was approved by the Regional Ethics Committee of Tampere University Hospital.
The baseline and follow-up study questionnaires were designed in co-operation with the Finnish Coeliac Society, patients with coeliac disease, and clinical researchers specialized in coeliac disease. The questionnaires included both free-text questions and questions with multiple options measured on a Likert scale. The baseline questionnaire comprised questions on sociodemographic conditions, duration, type and nuisance of coeliac disease-related symptoms prior to DH diagnosis and reactions to the diagnosis. In the case of coeliac disease-related symptoms, any symptom belonging to the wide symptom spectrum (GI and non-GI manifestations), was considered. The nuisance of symptoms was recorded with alternatives “a lot”, “a little”, “some”, “none” or “cannot tell”. The reaction to the diagnosis was assessed with alternatives “it was a shock”, “confused but confident”, “it was a relief” and “no effect”. Both questionnaires inquired into self-assessed personal health, concern for health, and use of healthcare services and pharmaceutical agents during the previous year. Self-assessed personal health was recorded on a 4-point scale with the alternatives “excellent”, “good”, “fair” and “poor”, and concern for health with the alternatives “extremely”, “moderately”, “a bit” and “not at all”. The follow-up questionnaire also asked about the strictness of the diet. Strictness of diet was recorded with 2 options: “strict diet” and “dietary lapses”.
Quality of life was evaluated with a self-administrated Psychological General Well-Being (PGWB) questionnaire. PGWB is a 22-item questionnaire, which has been validated and widely applied in coeliac disease research to assess quality of life and well-being (13–16). PGWB covers 6 emotional states: anxiety, depressed mood, self-control, positive well-being, general health, and vitality. All of the items use a 6-grade Likert scale, where value 1 represents the poorest and value 6 the best possible well-being. The total score of PGWB thus ranges between 22 and 132 points, a higher score indicating better quality of life.
The feasibility of the study questionnaires designed in co-operation with the Finnish Coeliac Society was pre-tested with a group of patients with coeliac disease who are members of the Society. Test-retest reliability was confirmed by having 11 treated patients with coeliac disease complete the same questionnaire one week after initial contact. The intraclass correlation coefficient was measured and the kappa values ranged from 0.84 to 1.00 (values above 0.70 are excellent). Cronbach’s α was not calculated as the test items were separated. All data were blindly coded before analysis.
All statistical analyses were performed with the IBM SPSS software, version 20 (IBM Corp. Released 2011, IBM SPSS Statistics for Windows, Version 20.0. IBM Corp., Armonk, NY, USA) in co-operation with a statistician. As the data were non-normally distributed, median values, minimum and maximum values and interquartile ranges were used to describe the continuous variables. All testing was 2-sided and p < 0.05 was considered statistically significant. A χ2 test was used in cross-tabulations, Wilcoxon signed-rank test for evaluating changes within groups and Mann-Whitney U test for assessing changes between groups.
The questionnaire was sent to 1,864 new members of the Finnish Coeliac Society, of whom 1,062 responded. At baseline 52 biopsy-proven newly diagnosed DH patients were enrolled, and 48 out of these 52 responded to the follow-up questionnaires after one year. The median age of the patients with DH at time of diagnosis was 52 years (range 23–74 years) and 35 patients were female (67%). The median age of the control group was 48 years (range 23–87 years) and 81% were female.
At diagnosis, the PGWB total score was significantly lower in DH patients (median 97, interquartile range (IQR) 83–107) compared with healthy controls (median 107, IQR 100–114) (p < 0.001), as were all PGWB subscores (data not shown). After one year on a GFD the DH patients’ PGWB total score increased significantly (median 106, IQR 94–113) and a statistically significant difference was no longer detected between treated DH patients and controls (p = 0.49); the only subscore that remained inferior for DH patients was general health (median 13, IQR 10–15 vs. median 15, IQR 13–16, p = 0.001).
When female and male DH patients were compared, the median duration of coeliac disease-related symptoms prior to diagnosis was significantly longer in females (4.5 vs. 2 years, p = 0.049). Female DH patients also had lower PGWB scores in total, depression and general health scores compared with male patients at time of diagnosis. However, after one year on a GFD, there was only a non-significant trend in vitality subscore towards decreased vitality in females (Table SI).
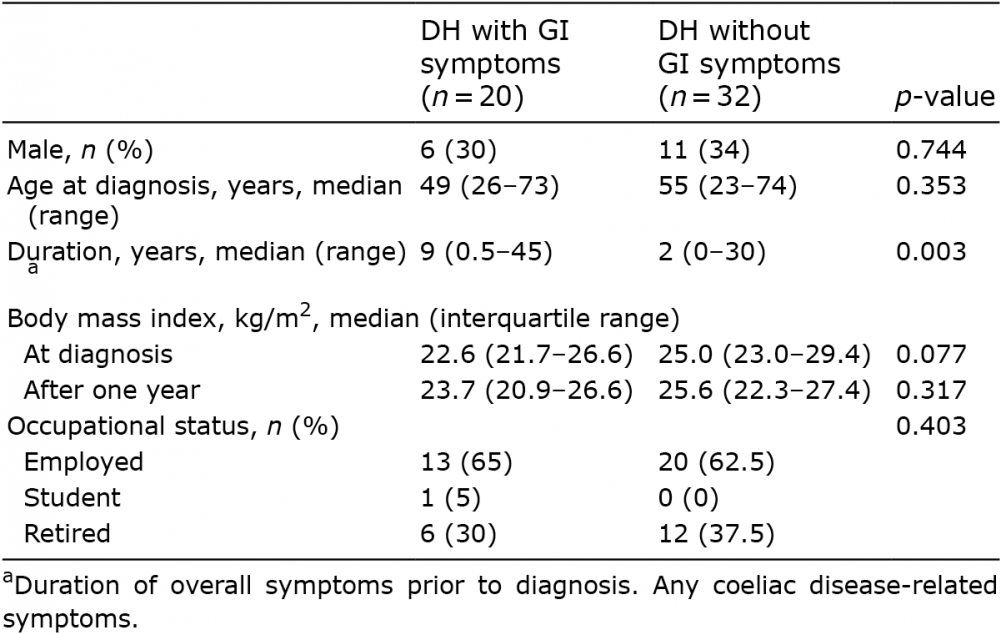
At time of diagnosis, 20 patients with DH (38%) reported having GI symptoms and 32 patients (62%) had no such symptoms. There were no differences in age, gender, body mass index (BMI) and occupational status between these 2 groups, but the median duration of coeliac disease-related symptoms was significantly longer in patients with DH with GI symptoms (9 vs. 2 years, p = 0.003) (Table I). One year after diagnosis, 94% of the DH patients with, and 90% of those without, GI symptoms were on a strict GFD.
Table I. Sociodemographic data and duration of symptoms prior to diagnosis in dermatitis herpetiformis (DH) patients with and without gastrointestinal (GI) symptoms
At diagnosis, the PGWB total score was significantly inferior in patients with DH with GI symptoms than among those with no such symptoms (Fig. S1). Also the well-being, self-control and vitality subscores were significantly lower in patients with GI symptoms (Table II). After one year of diet, the PGWB total scores had increased significantly in both groups and were at the same level as in healthy controls (Fig. S1). In PGWB subscores vitality and general health remained inferior in treated DH patients with GI symptoms compared with controls (Table II).
Table II. Median values and interquartile ranges for Psychological General Well-Being (PGWB) subscores in dermatitis herpetiformis (DH) patients with and without gastrointestinal (GI) symptoms at diagnosis and after one year on a gluten-free diet (GFD), and in healthy controls. A higher score indicates better quality of life
At diagnosis DH patients with GI symptoms significantly more frequently reported oral symptoms (25% vs. 3%), joint symptoms (35% vs. 3%) and weight loss (25% vs. 3%) compared with those free of such symptoms. The DH patients with GI symptoms were significantly more concerned about their health and reported inferior self-perceived health compared with those without GI symptoms (Table III) at time of diagnosis, while no significant differences between the groups were detected after one year on a GFD (Table III). Almost all DH patients found their symptoms disturbing at least to some degree at diagnosis, and all DH patients with GI symptoms and 93% of those without such symptoms were pleased to be diagnosed (Table III).
Table III. Subjective perceptions of symptoms, diagnosis, and health at time of diagnosis and after one year on a gluten-free diet (GFD) in dermatitis herpetiformis (DH) patients with and without gastrointestinal (GI) symptoms
DH patients with GI symptoms used, in general, more painkillers, medication for dyspepsia, sleeping medication and antibiotics than those without such symptoms within one year prior to, but not after, the diagnosis (Fig. 1). A significant difference was observed only in the use of antibiotics during the year prior to diagnosis. The use of healthcare services as all-cause consultations did not vary between the DH groups and the number of days of sickness absences from work were equal between groups both during the year prior to and after the diagnosis (Table SII).
Fig. 1. The percentage of dermatitis herpetiformis (DH) patients with and without gastrointestinal (GI) symptoms using pharmaceutical agents (A) during the year prior to diagnosis and (B) during the year after diagnosis on a gluten-free diet.
DH is an extraintestinal manifestation of coeliac disease presenting with troublesome, itching skin symptoms. A considerable burden of illness is related to itching
chronic skin diseases (11, 12), but research on the burden of illness in DH is scant. Previously, a small study (n = 10) showed that DH patients’ quality of life did not differ from that of healthy controls at the time of diagnosis, nor after one year of diet (17). In the present prospective study, we showed that DH patients’ quality of life at the time of diagnosis was inferior compared with that of the healthy subjects. However, if patients with DH were compared with the classical coeliac disease patients from the same series (6), the DH patients had better quality of life at diagnosis. We further detected an improvement in DH patients’ life quality after one year of GFD treatment, reaching the level of healthy controls in most values measured, and being superior to that in the classical coeliac disease patients from the same series (6). We have previously shown in a different series that DH patients’ quality of life is comparable to that of the healthy population even in the long term (18), which supports our present results.
In this study female patients with DH were found to have a poorer quality of life than male patients with DH. In our previous work, a similar decreased vitality was observed in long-term GFD-treated female patients with DH compared with male patients with DH (18). The same difference has been seen in classical coeliac disease: women have been shown to have a deteriorated quality of life compared with men (19, 20). The reasons for this gender difference in DH and coeliac disease are, thus far, unclear, but might be associated for example with challenges in everyday life, since women are, for example, more likely to be responsible for the planning and preparation of meals for the family (21). Female patients had a longer diagnostic delay in the current study compared with male patients, again as has been shown in coeliac disease (22). Furthermore, female DH and coeliac disease patients have been shown to have more severe GI symptoms than males (18, 23). The above-mentioned factors are also both linked to diminished quality of life in coeliac disease (5, 19, 24), and thus might offer other explanations for the gender differences in quality of life.
In addition to the skin symptoms, 38% of all patients with DH reported having GI symptoms at the time of diagnosis. In previous studies the prevalence of GI symptoms in DH cohorts has varied from 30% to none (3, 25–27). Since both patients’ and dermatologists’ primary focus is on the troublesome skin symptoms, there is a possibility that, especially milder, GI symptoms are ignored or not fully addressed. We showed that the presence of GI symptoms had a significant effect on the burden related to DH, as has been shown in coeliac disease (5, 19). DH patients with GI symptoms were more concerned about their health, perceived their health to be more deteriorated, and obtained lower scores in the PGWB questionnaire. DH patients with GI symptoms had also had longer diagnostic delay than DH patients without such symptoms. In addition, DH patients with GI symptoms presented overall a more heterogeneous clinical picture, demonstrated by the higher prevalence of additional oral and joint symptoms, and weight loss compared with DH patients without GI symptoms, this probably complicating the diagnostics and resulting in increased diagnostic delay. Interestingly, at diagnosis DH patients with GI symptoms had also used significantly more antibiotic treatments during the previous year than the DH patient without such symptoms.
Some limitations to the present study need to be discussed. In DH, the skin symptoms react slowly to GFD treatment alone, and therefore dapsone medication is often used in combination with dietary treatment to alleviate the skin symptoms more quickly (4). We had no data on the use of dapsone in our study population, and thus cannot verify the improved well-being in DH patients to be due solely to the GFD. We also used a generic quality of life questionnaire, which, although validated and widely used, is not designed specifically for coeliac disease or DH. In addition, by collaborating with the Finnish Coeliac Society we were able to recruit a fairly large and nationwide study cohort, although this might have caused selection bias. Also, in contrast to the known slight male predominance in DH (1), only 33% of the patients in this study were men. This may also have caused bias, since female patients with DH more readily perceive their quality of life to be poor compared with male patients. However, this does not explain the difference in quality of life between the DH patients with and those without GI symptoms, because the gender distributions were similar between the groups.
This study showed an impaired quality of life in DH at diagnosis and an improvement in the level of the healthy cohort after the first year on a GFD. At diagnosis, the presence of GI symptoms affected patients’ subjective perceptions of their well-being and was associated with an increased diagnostic delay and increased presence of other coeliac disease-related symptoms. In conclusion, closer attention should be paid to GI symptoms in DH.
This study was financially supported by grants from the Academy of Finland, the Sigrid Juselius Foundation, the Finnish Medical Foundation, the Foundation for Paediatric Research, the Mary and Georg Ehrnrooth Foundation and the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital (Grant numbers 9P060, 9P008, 9R018, 9S020, and 9R034).


 Click to show fullsize
Click to show fullsize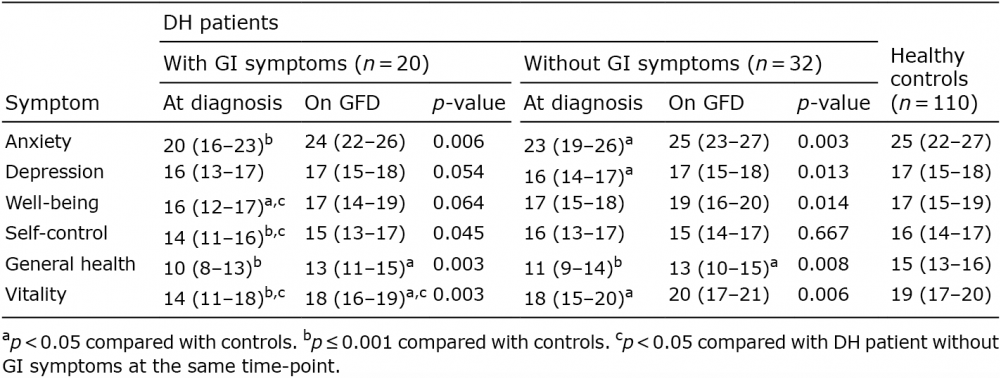 Click to show fullsize
Click to show fullsize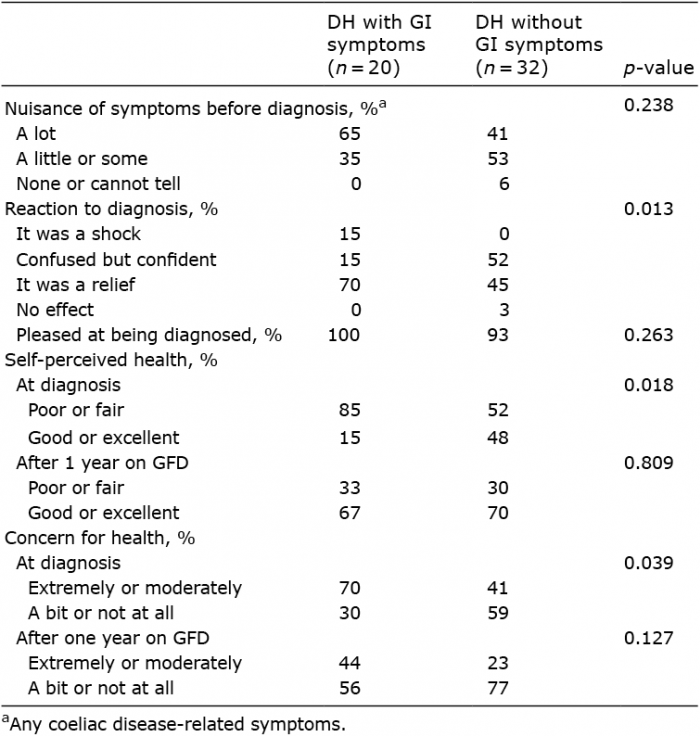 Click to show fullsize
Click to show fullsize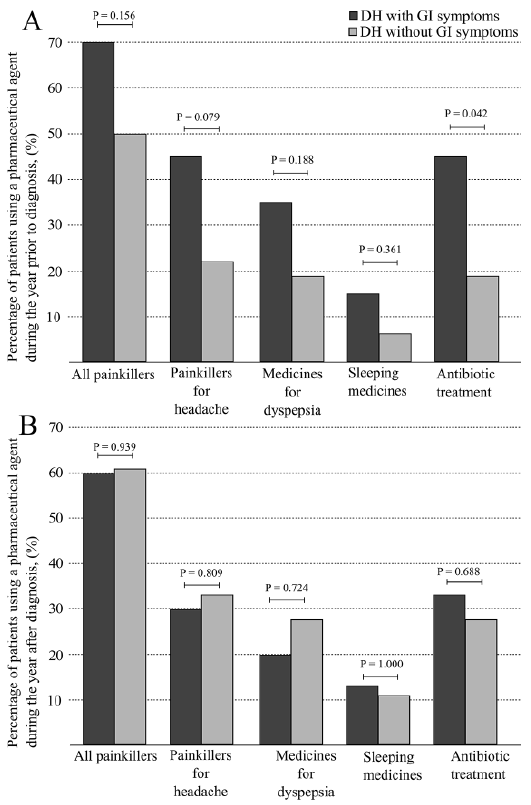 Click to show fullsize
Click to show fullsize