


1Fondazione ISTUD, Milano, 2DiSSal Sezione Dermatologia, Università di Genova/IRCCS AOU San Martino-IST, Genova, 3San Gallicano, Istituto Dermatologico -IRCCS- Roma, 4FederASMA e ALLERGIE, Prato, 5Dipartmento di Medicina Clinica Sperimentale, Dermatologia, Università di Messina, 6Immunoallergologic Unit AOU Careggi, Firenze, 7Dipartimento di Medicina Specialistica, Diagnostica e Sperimentale, Divisione di Dermatologia, Università di Bologna, 8UO di Dermatologia, Servizio di Allergologia, Policlinico di Modena, 9Dipartimento di Medicina, Università di Salerno, 10UOS Allergologia e Immunologia clinica, AO Luigi Sacco, Milano, 11Istituto di Dermatologia e Venereologia, Università Cattolica del Sacro Cuore, Roma, Italia, 12Lab. Immunologia e Allergologia- IDI IRCCS- Roma, 13UO Dermatologia, Dipartimento di Medicina Clinica e Sperimentale di Parma, Università degli Studi di Parma, 14Clinica Medica 1, Università di Padova, 15UOC di Dermatologia Universitaria “Daniele Innocenzi” Università degli Studi di Roma Sapienza Polo Pontino, 16Allergy Unit, Università di Verona e Ospedale Generale, Verona, 17Clinical Allergological and Venereological Section, Medicine Department, University of Perugia, 18Clinica dermatologica, Università degli Studi di Tor Vergata, Roma, 19Clinica Dermatologica, Ospedale Maggiore, Trieste, 20Azienda Ospedaliera San Carlo, Potenza, 21Ospedale Papardo, Messina, 22Dipartimento di Scienze Biomediche ed Oncologia Umana, Clinica Dermatologica, Policlinico di Bari, 23UO Dermatologia Allergologica, Dipartimento di Chirurgia e Medicina Traslazionale, Azienda Sanitaria e Università di Firenze, 24Unità di dermatologia, Dipartimento di neuroscienze, salute mentale e organi sensoriali Università la Sapienza, Roma, 25Clinica dermatologica, Università degli studi di Roma “Sapienza”, Policlinico Umberto I, Roma, and 26Novartis Farma, Origgio, Italy
Chronic spontaneous urticaria (CSU) is perceived as a difficult to manage disease with negative impact on quality of life. The aim of this study was to highlight how to improve the care of people with CSU, using the methodology of narrative medicine. From June 2014 to March 2015, CSU-diagnosed patients and their physicians were asked to record their experiences of the condition in writing. Fourteen healthcare teams participated: 41% considered CSU as a challenge to overcome, while 22% experienced CSU as a big commitment. The number of professional involved was evaluated as insufficient in 11 hospitals. Seventy-five percent of the 190 Italian patients had visited 3 or more physicians before receiving a final diagnosis, with a perceived waste of time and resources. The therapeutic pathways were described as unsatisfactory in 83% of cases. As a result, anger and frustration were life-dominant emotions in 92% of patients. The critical points of the care pathway are related to organizational issues and lack of awareness.
Key words: narrative medicine; urticaria; quality of life; quality of healthcare.
Accepted May 30, 2016; Epub ahead of print Jun 8, 2016
Acta Derm Venereol 2017; 97: 81–85.
Corr: Antonietta Cappuccio, Fondazione ISTUD, Piazza IV Novembre 7, IT-20124 Milano, Italy. E-mail: acappuccio@istud.it
Urticaria is characterized by the sudden appearance of itchy wheals, angioedema, or both (1), with an unpredictable pattern that prevents patients from planning their life on a daily basis. Based on the duration of symptoms, urticaria is distinguished as acute and chronic (2), defining chronic urticaria (CU) as the daily (or almost daily) manifestation of symptoms for a period of over 6 weeks (2). This is further classified into 2 subgroups: inducible urticaria, triggered by recognizable environmental or physiological factors (e.g. low temperatures, heat, pressure, or exercise) and chronic spontaneous urticaria (CSU), which appears not to be triggered by any recognizable external factor (3).
According to recent studies, CU affects 0.5–1.0% of the population, with CSU accounting for approximately two-thirds of the total cases (4).
From a clinical point of view, CSU is difficult to manage (5) and several evaluations may be required before a diagnosis is reached, often causing frustration among people affected and a waste of economic resources in their search for a solution (6).
Despite the disease impacting heavily on patients’ quality of life (QoL) and interpersonal relationships (7), until recently psychological and social aspects have remained a secondary, underestimated (8), issue. An increasing number of studies are addressing QoL in relation to the potential benefits provided by therapies (9), and its evaluation has been included in the current version of the EAACI/GA2LEN/EDF/WAO guidelines (1).
The narrative medicine approach seeks to understand the patient–clinician relationship through the collection and analysis of narratives, told from the standpoint of the many stakeholders involved: patients, health and social professionals, and family members (10). This practice uses methods to gain insight into how a person lives with his/her illness, in an attempt to consider the many facets of the pathway of care (11).
Narratives allow professionals to collect information on the needs perceived by patients and physicians when coping with distress caused by clinical problems, which cannot be collected by traditional methods, such as structured questionnaires (12). Many physicians are experimenting with narrative medicine, witnessing its validity in changing clinical practice, either in reducing anxiety and insecurities in both patients and professionals or revealing gaps in disease treatment, patient support and care or other factors (13). From an organizational and economic point of view, narrative medicine can be used as a systemic approach to improve the efficacy and efficiency of healthcare services (14).
The aim of the current study was to stimulate reflection on behalf of the immunologists, dermatologists and allergists involved in the care of patients with CSU, by means of the collection of narratives from patients and healthcare professionals. In particular, this study focused on the lives of people with CSU, and on medical, emotional, and relational aspects of the disease acquired through the methodology of narrative medicine.
The ultimate aim of this project was to identify the critical steps in the CSU caring process and to find new solutions to improve this process.
The study was performed in Italy from June 2014 to March 2015. Patients were invited to record their experiences with CSU in writing through a promotional campaign in several national newspapers, social media (internet) and through the collaboration of 25 dermatological/allergy Italian centres, by means of informative posters and brochures placed in the waiting rooms.
Inclusion criteria for patients were: (i) having and coping with urticaria for a period of at least 6 weeks or more; (ii) a diagnosis of CSU, as defined by the EAACI/GA2LEN/EDF/WAO guidelines; (iii) the ability to read and write in Italian; and age over 14 years.
Patients were invited to access the website www.medicinanarrativa.eu/orticaria and narrate their personal experience, based on the prompts provided by a semi-structured narrative plot tracing a chronological description of events. Narrative plot was developed so as to allow researchers to verify whether patients were truly affected by CSU and discriminate them from the narratives left by patients affected by inducible CU (see Appendix S1). Conversely, physicians were directly approached by researchers after drawing from a selection of centres chosen based on the number of CU patients treated and geographical location throughout Italy. Physicians were administered a quantitative questionnaire as well as a semi-structured questionnaire on professional experience in general and in managing patients with CSU (see Appendix S2).
Narratives were collected through the Typeform online survey platform (15). Raw and anonymous results were downloaded as a Microsoft Excel spreadsheet. All data were self-reported and submitted anonymously.
All survey instruments received prior approval by a multidisciplinary Scientific Board, which was involved in discussing the results and which contributed actively through a qualitative consensus meeting. Moreover, prior to the beginning of the study, notification was given to all ethics committees or medical management of the centres involved, and all patients and health professionals provided written informed consent. The project was performed in accordance with the principles of the Declaration of Helsinki.
Based on the Italian prevalence of CU, rates of observed patterns from 190 narratives of patients ≥ 85%, were considered statistically significant with a confidence interval equal to 95%.
Socio-demographic variables were analysed with descriptive statistics (mean and ranges, and classes) and frequencies reported as percentages.
Narratives, written in the local language (Italian), were analysed using an approach integrating qualitative and quantitative research, which consist in the qualitative interpretation of stories, through triple-blind reading by 3 independent researchers, to reduce bias in the interpretation of texts (16). Quantitative analysis was carried out using specific software; NVivo (17) (see Appendix S3), which enabled the calculation of word frequencies (12).
The text analysis took into consideration: classification of the pathology into disease, illness, and sickness (18); emotional analysis (19); and Frank’s classification of illness narratives (20).
The online database was accessed by a total of 1,810 people, of whom 199 patients (10%) with CU submitted a written narrative about their experiences. Nine narratives were excluded as they were from patients with inducible CU. The basic sociodemographic characteristics of the participants are summarized in Table SI. Distribution of males and females was in line with the prevalence of urticaria among the Italian population (21), and mean disease duration was 7 years (range 2 months to 54 years).
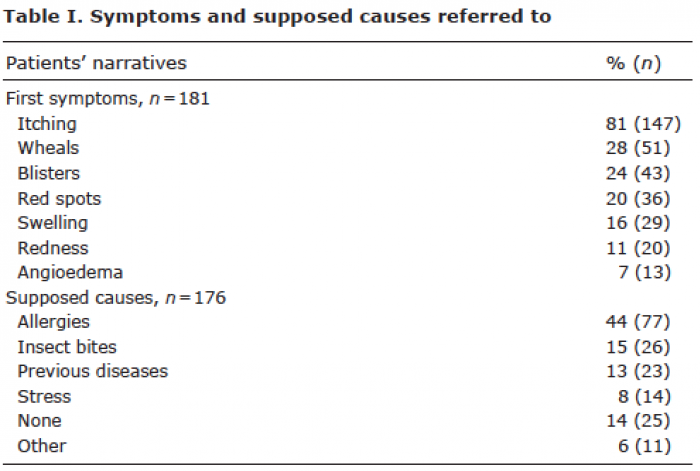
Onset of symptoms and diagnosis. Symptoms described by patients in narratives were in agreement with those reported in the literature (Table I). Symptoms were most often referred to (see Table SII) as metaphors representing the concepts of fire (32%), needle and insect bites (28%), and loss of control over the body (24%), and were often linked to a specific cause, except in 14% of cases (Table I).
Table I. Symptoms and supposed causes referred to
In 45% of cases the first healthcare professional the patient referred to was their general practitioner (GP); however, the diagnosis of CSU in 70% of cases was established by a dermatologist or an allergist (Table II).
Table II. Healthcare professionals (or similar) to whom patients referred to for the first consultation and who made the diagnosis
The emotions felt by patients upon communication of the diagnosis were negative in 84% (mostly due to the lack of a clear cause and a cure), relief in 8% (finally a name for their disease), and neutral in 8% (they had already suspected/knew what they were suffering from).
Relating to health professionals and the pathway of care. Waste of resources throughout a seemingly erratic path of care was a recurrent theme. Seventy-five percent of the population had consulted at least 3 physicians and 55% had been to the emergency room at least once. In addition, 67% of patients affected by CSU reported a sense of frustration, having had to repeatedly undergo diagnostic tests in the search for a cause.
Only 14% of written experiences portrayed a positive entrusting patient–physician relationship based on reassurance of the existence of a cure and the physician’s empathic attitude.
Although patients were asked not to name the therapy followed, 88% of the narratives still addressed this topic as being a pivotal element.
When asked to recall the path of care faced, 83% of people living with CSU expressed having experienced negative feelings. For 26% of people discomfort and frustration eventually led them to give up seeking further specialist consultations, opting instead for self-care and turning to the GP only for drug prescriptions.
Emotional experience and everyday relationships. Feelings prevalent throughout the narratives were: anger, as the chronic life-dominant emotion (92%), followed by fear (67%), and shame (64%). Some narratives also highlighted the almost total lack of psychological support (5%) or complementary treatments to control stress and anxiety.
Family relationships were dominated by fear and anger in 79% of narratives, and revealed 2 opposite reactions: either underestimation of the disease on behalf of their family in 43% of cases, or exaggerated concern in 36% of cases.
On the other hand, in referring to relationships and interactions outside the household, 86% described negative feelings of shame (60%), pain (15%) and anger (11%).
In referring specifically to relationships in the workplace, 30% of narratives described a sense of embarrassment, 54% as an obstacle in continuing their job because of the reported condition and the lack of understanding.
Living with urticaria “today” and hopes for the future. In the final section of the plot, narratives addressed the person’s perception of life today and their hopes for the future. Eighty-five percent described a general impairment in QoL, though with different shades and nuances; of these 36% described life with CSU as difficult, 39% described the disease using exasperating phrases and metaphors (e.g. “a true agony” or “a terrible nightmare”) and 15% described CSU as an inescapable and difficultly acceptable reality. Alongside these stories of discomfort, 10% of narratives expressed acceptance of the disease and the finding of new ways to manage their daily lives.
With reference to thoughts for the future, only 46% of people still hoped for an improvement. However, 54% of patients viewed the future as being the same as, or worse than, the present, with continuous anxiety around the onset of symptoms.
With reference to how CSU should be treated, 57% of patients hoped for a simpler and faster treatment process, especially with regard to diagnosis. Twenty-seven percent of patients, however, clearly requested a permanent cure for hives, 10% asked for greater awareness from both primary care physicians and society, and 6% mentioned more investment in research.
Experience of writing and classification of the narratives. According to the classification by Kleinman, the most recurrent terms were associated with the disease (96%), and therefore with the mechanistic view of CSU. In the study population, 77% of narratives were stories of chaos. Twelve percent of narratives were identified as restitution, while 10% were quests, typical of chronic disease.
To the question about how participants felt about this narration experience, our results evidenced a feeling of usefulness, with the hope that the project would eventually help to find a cure, as well as gratitude for having the opportunity to express themselves freely and finding a listener.
Of the 25 centres participating in the project, 14 teams (56%) responded to the questionnaire, with a total of 33 healthcare professionals involved. As reported in Table SIII, only 3 teams (21%) considered the number of professionals assigned to CSU at their centre as adequate and 21% as poor; most (86%) claimed the contribution of the psychologist in their facility was either lacking or insufficient.
Fifty percent of the healthcare professionals were not satisfied with the care provided to their patients, and no participant was completely satisfied. All teams stated that they did not interact with GPs and reported a lack of any relationship with this category. The actions health professionals proposed in order to improve the management of CSU are summarized in Table III.
Table III. Elements that health professionals (n = 33) consider important towards improving management of chronic urticaria
The motivation leading healthcare providers to become a doctor/nurse were passion or interest in the topic in 61% of cases, see Table SIV. In describing how professionals viewed CSU and how they felt in dealing with the management of this disease, 41% described the disease as challenging to defeat, and 22% as a big commitment that requires time and dedication. The remaining 36% described themselves as benefactors in dealing with CSU.
Thirty-one percent of care providers envisioned their future with difficulty or with some suggestions for improvements, and 42% as a path that would eventually be peaceful thanks to their commitment.
The aim of this study was to gain perspective on the impact of CSU on people’s lives and their experience from symptom onset, to diagnosis, and thereafter. Al-though several studies have reported on QoL, these have mainly investigated the issue using traditional methods (8). Findings from our study using a narrative method enabled us to uncover new or previously underestimated aspects of living with CSU.
Narratives written by people affected by CSU feature a dominant feeling of anger, with 92% claiming daily challenges in managing the disease and a burden caused by this feeling. These findings are in line with the results of the QoL assessment for urticaria, in which aggressiveness and frustration show high scores (6), but are higher than for other dermatological diseases, such as psoriasis (22). Based on the results of questionnaires reported in the literature, the major causes of impaired QoL are itching and wheals (23). This is also found across narratives; moreover, symptoms are often aggravated by spasmodic and repetitive scratching.
The analysis of narratives evidences the difficulties of living with CSU. In 79% of cases relationships with family members were neither serene nor comforting, and in 60% of cases relationships with the outside world were restrained by a feeling of shame. As with psoriasis, shame was directly associated with widespread prejudice in others, fear of being rejected, and eventually with a desire to “hide” the most evident symptoms (24). Such feelings heavily affected the relational and intimate dimension and inevitably hindered professional performance (25).
Other recurring themes are feelings about the search for a treatment, the doctor–patient relationship, and the impact of these on patients’ acceptance of the disease. Patients’ narratives put much emphasis on the frustration deriving from their pathway of care. In 83% of cases the pathway was described as unsatisfactory, and in 75% of cases it involved consultation with more than 3 physicians before a diagnosis was reached or appropriate treatment found. The inadequacy of the pathway of care also found correspondence in the physicians’ narratives, with many physicians highlighting the lack of dedicated, multidisciplinary teams and inadequate training of GPs (who were the first referral for over 50% of patients) on CSU. On the other hand, this organizational gap is clearly perceived by patients, who openly expressed doubt that they were being referred to the right specialist. In fact, this would be partially explained by the fact that CSU is currently classified as a skin disease, but may be diagnosed by either a dermatologist or allergist and eventually be treated by the allergist.
Another common point is the lack of a psychologist, whose support might help patients to cope with the disease. This can boost the person’s self-confidence and improve social interactions. Psychological support is also recommended by recent studies that show a correlation between CSU and psychiatric comorbidity (26) and, in general, a psycological support is always recommended when a dermatological disease arise (27). It should be noted, however, that patients who succeeded in coping with the disease were those who encountered physicians who simply listened to them and put an effort into creating a long-term doctor–patient relationship based on honesty and trust, as also described in previous studies (28).
Taken together, these gaps in patient management and the lack of a structured pathway of care clearly reveal a large amount of waste of both private and public resources on inappropriate medical tests and consultations. Although the economic issue was not directly addressed by this study, these findings provide evidence of critical flaws in the healthcare system, which can be used towards a more rational organization and allocation of economic resources.
The findings of this study must, however, be considered in the light of potential bias. The project foresaw open participation, in which patients freely decided to provide their testimony. However, this may have encouraged participation among the most unsatisfied, and angriest, patients, who found in this project a forum for their complaints. Yet, the 92% of concordance on anger remains a strong signal, which cannot be neglected in clinical and social settings. A profound need for more compassionate caring by the physician, adequate psychological support, and social awareness of the disease emerges from these findings. These objectives can probably be reached
through proper training of the professionals involved and through informative campaigns to shatter preconceptions and stigma around CSU.
Another limitation may be represented by the geogra-phical origin of the data. Although the data are quite representative of the European setting and probably transferable to other European countries with similar anthropological heritage and healthcare systems, future investigations should, nevertheless, be extended to other countries.
The authors are grateful to Manuella Walker and Alessandra Fiorencis for editing the manuscript.
The project was supported by an unconditional grant from Novartis Farma Italy.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize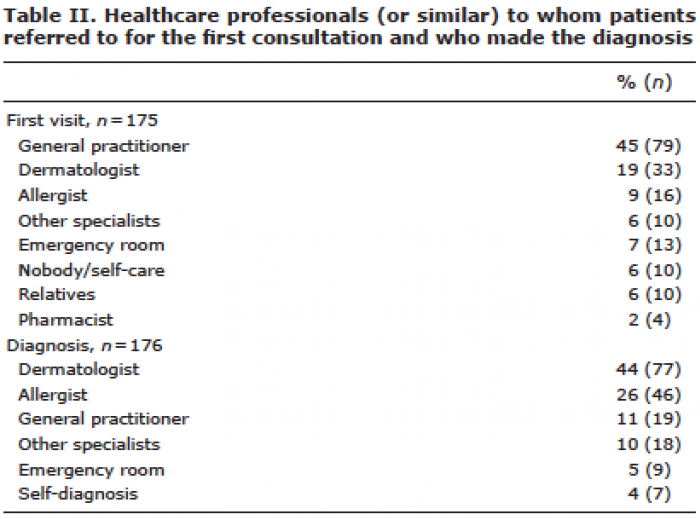 Click to show fullsize
Click to show fullsize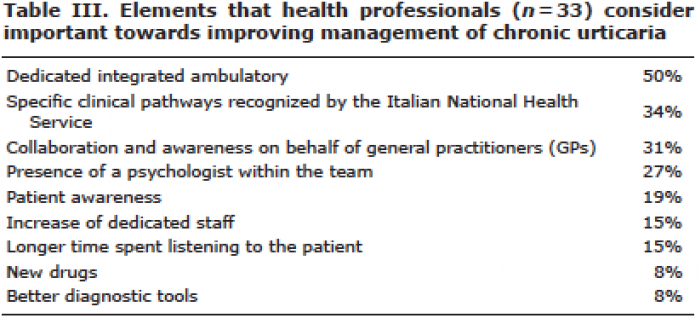 Click to show fullsize
Click to show fullsize