


Department of Dermatology, University of Parma, via Gramsci 14, IT-43100 Parma, Italy. E-mail. fra.satolli@libero.it
Accepted Jul 24, 2017; Epub ahead of print Jul 24, 2017
Basal cell carcinoma (BCC) is the most common malignancy in humans and it usually occurs as a solitary lesion on sun-exposed areas. Its association with non-organoid epidermal naevi (NONEEN) is an uncommon event. To our knowledge, there have been very few cases reported in the literature so far, and, among these, only two cases of multiple BCCs arising in a verrucous epidermal naevi (1, 2).
We report a case of a 73-year-old woman affected by multiple BCCs that have arisen within the context of a congenital verrucous epidermal naevus of the left thigh and left foot. We investigated the possible role of genetic mutations.
The challenge was also to find an effective treatment for BCCs, considering the multiplicity of lesions. There-fore, we also used some off-label treatments, such as ingenol mebutate, which resulted in partial clearance.
During follow-up, the patient also developed a superficial melanoma on the same leg as the verrucous epidermal naevus.
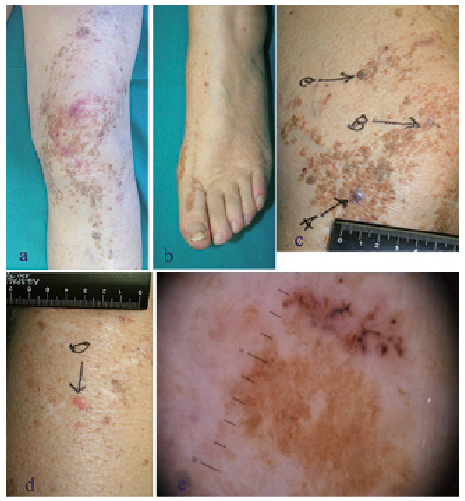
A Caucasian woman in her seventies was referred to our department because of the recent appearance of about 30 pinkish-purple or pigmented papulo-nodular lesions within the context of a pre-existing congenital verrucous epidermal naevus of the left leg (Fig. 1a, b). Clinical and dermoscopical examinations (Fig. 1e) revealed features of BCCs.
Fig. 1. Clinical characteristics. The congenital verrucous epidermal naevus (a, b). The surgically excised BCCs arising within the nevus’ (c, d). Dermatoscopic evaluation of BCCs showed in detail large blue-grey ovoid nests or blotches, structureless of leaf-like areas (e).
We decided to surgically remove the 4 largest lesions (Fig. 1c, d). Histopatho-logical examination showed acanthosis, papillomatosis and hyperkeratosis, typical of non-organoid non-epidermolytic epidermal naevi and, in this context, also nests of basaloid cells with a palisade pattern and hyperchromatic nuclei diagnostic of BCCs (Fig. S1a). Immunohistochemistry with BerEP4 confirmed the diagnosis of BCCs (Fig. S1b).
Although the patient had neither the clinical features of a naevoid basal cell carcinoma syndrome (such as palmar pits, keratocystic odontogenic tumours, skeletal anomalies, ectopic calcifications or macrocephaly) nor a family history for the syndrome, we decided to investigate the PTCH1 gene to exclude the diagnosis of mosaicism in Gorlin syndrome.
Molecular examination with PCR and DNA sequencing revealed no pathological mutations in the PTCH1 gene. However, a different mutation located in the 5th untranslated region (UTR) of PTCH-1 was found and considered.
During the last 5 years of follow-up, the patient developed 47 BCCs which occurred in a linear naevus. Moreover, she developed a superficial melanoma IA (according to AJCC 2009 staging guidelines for melanoma (3) Fig. S2) on the same leg that was treated surgically (by excisional biopsy and wide excision).
At each subsequent visit, both surgery and photodynamic
therapy using methyl aminolevulinate (MAL-PDT) were offered to the patient to remove the remaining lesions but she determinedly refused due to the pain and suffering caused by these procedures. We therefore used imiquimod 5% cream once a day, 5 days a week for 6 weeks, thereby achieving partial clearance of the lesions; the smaller ones were treated with cryotherapy (two cycles of 30 s each one) which was shown to be effective but painful. We also tested ingenol mebutate gel during the last year; she applied a dose of 500 µg for 3 consecutive days a week for 3 weeks, with a poor response, but without adverse effects. Given the greater efficiency of Imiquimod, we decided to try it again, with the same posology and adding an occlusive dressing. The use of imiquimod under occlusion resulted in a complete clinical resolution of the BCCs.
BCC can occur as a sporadic feature or in several genetic syndromes. Among these, the most commonly known is Gorlin syndrome (or nevoid basal cell carcinoma syndrome, NBCCS), an autosomal dominant trait caused by a mutation of the PTCH gene at 9q22.3 (4).
Despite our patient did not suffer from any of the developmental defects described for NBCCS, given the development of multiple BCCs, we investigated the PTCH gene to exclude Gorlin syndrome.
Although pathological mutations for PTCH in translated regions have not been found, a mutation in the 5th untranslated region has been observed. This mutation, characterised by 8-fold CGG repeats in the 5’UTR, is the subject of debate in the literature. Some authors (5) did not find an increase in frequency in the development of sporadic BCCs associated with this mutation. However, other authors (6, 7) have suggested the possibility of a predisposition to BCC by a non-coding mutation in the 5’UTR with 8 CGG repeats. The result of our molecular investigations favours the latter.
As also proven by our case, not all instances of multiple BCCs are due to genetic syndromes. Happle (4), reporting a study made of Guarneri et al. (8) (concerning 3 cases of multiple BCCs in 3 successive generations of a family) postulated that multiple superficial BCCs without associated anomalies are distinct from the Gorlin syndrome and could be explained by an autosomal dominant phenotype (4). Alternatively, this non-syndromic phenotype might have a polygenic basis. Furthermore, a recent article (9) has revealed that multiple BCCs can be also part of the BAP 1 mutation.
Of particular note in this case, is the development of BCCs on an epidermal naevus, an event that is per se infrequent. The verrucous epidermal naevi represent today a paradigm for cutaneous mosaic disorders (10). To our knowledge there are only two cases (1, 2) in the literature of multiple BCCs arising with the context of a linear epidermal naevus (Table SI1) (11).
Hafner et al. (11), analysing PIK3CAA and FGFR3 mutations, suggested that both lesions (BCC and NONEEN) might share a common, but as yet, unknown genetic molecular alteration or, more likely, they may result from a distinct clonal origin.
Other issues have arisen in this case. Firstly, the appearance of a superficial melanoma on the same leg of the epidermal verrucous naevus and of multiple BCCs. A recent study (12) has revealed that individuals with multiple BCCs have a significantly higher proportion of squamous cell carcinomas and/or melanomas compared to those with a single BCC. The second issue to arise is the choice of treatments for BCCs. This was a challenge because of the high number of BCCs that had developed and the refusal of the patient to undergo surgery, MAL-PDT and radiotherapy treatments, due to pain. Only one similar case has been described in literature (13) where aminolevulin acid photodynamic therapy, cryotherapy, and chemotherapy with 5-fluorouracil (5-FU) were attempted. In our case, we opted to test imiquimod 5% cream, cryotherapy and ingenol mebutate gel. In terms of tolerance to the therapy and the clinical disappearance of the lesions, the best treatment proved to be with imiquimod 5% gel applied to the area with an occlusive dressing. The follow-up period after treatment was once every month for the first 6 months, then every two months.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize