


Departments of Dermatology: 1Stavanger University Hospital, Stavanger, Norway, 7Justus Liebig University, Giessen, Germany, 8ULB-Erasme Hospital, Brussels, Belgium, 9Zealand University Hospital, Roskilde, Denmark, 10University Hospital of Brest, Brest, France, 14Oslo University Hospital, Rikshospitalet, 15University of Oslo, Oslo, Norway, 18Russian National Research Medical University Pirogov, Moscow, Russia, 19Royo Villanova Hospital, Aragon Health Sciences Institute, Zaragoza, Spain and 20Sisli Etfal Teaching and Research Hospital, Istanbul, Turkey, 2Department of Dermatology and Wound Healing, Cardiff University School of Medicine, Cardiff, UK, 3Institute of Medical Psychology, Justus Liebig University, Giessen, Germany, 4Department of Psychology, University of Zaragoza, Aragon Health Sciences Institute, Zaragoza, Spain, 5National Norwegian advisory board for concurrent addiction and mental health problems, Innlandet Hospital Trust, Brumunddal, 6Department of Public Health, Innlandet University College, Elverum, Norway, 11Department of Dermatology and Allergology, University of Szeged, Szeged, Hungary, 12Clinical Epidemiology Unit, Istituto Dermopatico dell’Immacolata, Rome, Italy, 13Health, Medical and Neuropsychology Unit, Faculty of Social and Behavioural Sciences, Leiden University, Leiden, The Netherlands, 16Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland, 17Moscow Scientific and Practical Centre of Dermatovenereology and Cosmetology, 21School of Life & Medical Sciences, University of Hertfordshire, Hatfield, 22Institute for Medicines Development Cardiff, UK, and 23Department of Dermatology and Venereology, Skåne University Hospital, Lund University, Malmö, Sweden
Skin disease and its therapy affect health-related quality of life (HRQoL). The aim of this study was to measure the burden caused by dermatological therapy in 3,846 patients from 13 European countries. Adult outpatients completed questionnaires, including the Dermatology Life Quality Index (DLQI), which has a therapy impact question. Therapy issues were reported by a majority of patients with atopic dermatitis (63.4%), psoriasis (60.7%), prurigo (54.4%), hidradenitis suppurativa (54.3%) and blistering conditions (53%). The largest reduction in HRQoL attributable to therapy, as a percentage of total DLQI, adjusted for confounders, was seen in blistering conditions (10.7%), allergic/drug reactions (10.2%), psoriasis (9.9%), vasculitis/immunological ulcers (8.8%), atopic dermatitis (8.7%), and venous leg ulcers (8.5%). In skin cancer, although it had less impact on HRQoL, the reduction due to therapy was 6.8%. Treatment for skin disease contributes considerably to reducing HRQoL: the burden of dermatological treatment should be considered when planning therapy and designing new dermatological therapies.
Treatments for skin diseases differ from those used for other diseases. They may be messy, time-consuming, affect clothing or be painful. Some diseases are burden-some (psoriasis, eczemas, itching) and their therapy causes extra impairment, which should be appreciated. Others showed little impact from therapy, although the diseases themselves were serious (hidradenittis suppurativa, psycho-dermatological conditions, acne). Adequate therapy should be sought to alleviate symptoms without adding further impairment. Lastly, some skin diseases stood out as more burdened by therapy than by the disease itself (cancer, allergies, scars). For these patients, choice of therapy is most important for providing optimal help.
Key words: quality of life; HRQoL; DLQI; dermatological therapy; burden of skin disease; therapy burden.
Accepted Mar 1, 2018; Epub ahead of print Mar 2, 2018
Acta Derm Venereol 2018; XX: XX–XX.
Corr: Flora Balieva, Department of Dermatology, Stavanger University Hospital, Pb. 8100, NO-4068 Stavanger, Norway. E-mail: florabalieva@gmail.com
Topical and other dermatological therapies can add to the burden of skin disease, as they may be time-consuming, messy, intervene with clothing choice, and impact on health-related quality of life (HRQoL) in ways that are unique to the skin (1, 2). This contrasts with the relatively low burden of oral therapy in other diseases (3) where, for most, oral medication becomes routine. However, even systemic dermatological medications, such as cytotoxic drugs, corticosteroids, retinoids, intravenous or injected biologics, may have an associated burden. Topical and injection routes of drug administration have the lowest levels of convenience and global satisfaction (4).
Impairment of HRQoL due to dermatological therapy is little explored, even though the burden caused by skin disease treatment is very important, both to patients and because it contributes to poor adherence (5).
Most generic measures of HRQoL were developed with-out including skin diseases. It is therefore unsurprising that they miss the burden experienced by dermatological patients. In measures designed for use across skin diseases, only the Dermatology Life Quality Index (DLQI) includes a question concerning the impact of treatment on everyday life (6).
The aim of this study was to measure how therapy for skin disease contributes to reducing HRQoL in outpatients across Europe.
Data were obtained from a cross-sectional multicentre study on patients recruited from 15 dermatological outpatient clinics in 13 European countries: details have been previously reported (7). The study was approved by the Regional Committee for Medical Research Ethics in Norway. Separate ethical approvals were obtained where necessary. The study was conducted in accordance with the Declaration of Helsinki.
Consecutive patients, age over 18 years, understanding the local language and not having severe mental disease were invited to participate on random days, giving written consent. Participants completed questionnaires on sociodemographics (sex, age, ethnicity, education, marital and socioeconomic status), the DLQI and other questionnaires (7–11).
Patients were examined by the dermatologist, who recorded comorbidities: diabetes mellitus, cardiovascular, chronic respiratory, rheumatological or other disease. Workers from each hospital’s service division were invited to participate as controls.
The DLQI, a 10-item questionnaire, was used to assess impairment in HRQoL. Question 10, which concerns the impact of therapy, was used to assess how treatment impaired HRQoL: “How much of a problem has the treatment for your skin been, for example by making your home messy, or by taking up time?” with possible answers “very much” (scored 3), “a lot” (2), “a little” (1) or “not at all/not relevant” (0).
The DLQI was not designed for use by healthy individuals. Patients with naevi (n = 192) served as “healthy” controls, since there were no significant differences between the patients with naevi and healthy controls (7, 8).
Data from all centres were merged. Diagnoses were organized into 35 disease groups (8, 12).
SPSS 24 software was used for statistical analysis. Frequencies and means for patient and control characteristics were calculated.
The answers to DLQI question 10 were dichotomized into “no impairment” (0) or “impaired” (1, 2 or 3) when calculating frequencies of positive answers.
For each diagnosis the mean scores for question 10 and total DLQI were calculated. Their relationship was calculated as
, denoted as Q10%.
Comparisons between patients with naevi and healthy controls were performed with the t-test for continuous variables (age) and the χ2 test for categorical variables (sex, marital status, socioeconomic status, comorbidities, economic difficulties, stress, depression and anxiety (7)) and linear (EQ-VAS) and logistic regressions (EQ5D) for comparing HRQoL outcomes (8).
Linear regression was performed to analyse Q10% for each diagnosis, adjusting for age, sex, socioeconomic status and comorbidity with “naevi” as controls.
A search for publications on therapy issues in dermatology using DLQI or other instruments was performed using MEDLINE, EMBASE and Cochrane Library following standard search strategies. Search terms and medical descriptors (MeSH) included skin disease, dermatosis, dermatoses, quality of life, DLQI, skin therapy, topical therapy, photodynamic therapy, cryotherapy, cryosurgery, cryoablation, laser, phototherapy, photochemotherapy, ultraviolet B (UVB), UVA, UVA1, psoralen plus UVA (PUVA), retinoid plus PUVA (RePUVA), topical drug administration, parenteral administration, biological therapy, tumour necrosis factor (TNF)-α inhibitors, infusion therapy, skin cancer therapy, and surgical dermatological therapy.
There were 4,010 participants and 1,359 healthy controls. Comparative details have been published previously (7–11) and are given briefly in Table SI.
There were 3,846 (96%) valid answers to DLQI, 5.2% of which had a DLQI > 20 (extremely large effect on HRQoL). One-fifth (20.3%) experienced at least a very large effect (DLQI > 11) and 44.9% had a DLQI > 6, meaning at least a moderate effect on HRQoL (13) caused by their skin disease (Table I).
Table I. Frequencies of Dermatology Life Quality Index (DLQI) scores (n=3,846)
The total patient population (n = 3,846) had a mean ± standard deviation (SD) DLQI score of 6.7 ± 6.8, meaning moderately impaired HRQoL. Except for naevi, no skin disease had a mean score < 2, so all had at least a small effect on patients’ HRQoL. Twenty-seven of the 35 (77%) skin conditions had mean DLQI scores > 5, indicating at least a moderate effect on a patient’s life (Table SII).
Higher DLQI values, indicating higher impairment, were seen in females, younger age groups, patients with comorbidities and those with lower socioeconomic status.
Question 10 in the DLQI addresses therapy-related issues. The numbers of patients answering with “a little”, “a lot” or “very much”, i.e. other than “no impact/not relevant”, are given in Fig. 1. More than half of the patients with atopic dermatitis (AD) (63.4%), prurigo (60.7%), psoriasis (54.4%), hidradenitis suppurativa (HS) (54.3%) or blistering disorders (53%) answered positively. Fifteen of 32 skin conditions had > 33.3% patients scoring positively.
Fig. 1. The percentage of positive answers to having therapy issues (Question 10 of the DLQI) for each diagnosis. Diagnoses represented by fewer than 20 valid answers (hyperhidrosis (12), nail diseases (17) and granuloma annulare (13) excluded). NMSC: non-melanoma skin cancer.
The mean scores with SD for question 10 and Q10% for each diagnosis are presented in Table II. There are no existing cut-off values for interpreting results from single questions of the DLQI, and isolated values may not give a clear perspective as to how large the impact is. Q10% is not a standardized method for interpreting DLQI data, but does provide perspective on how therapy issues relate to the total HRQoL impairment. Table II lists the diseases in descending values according to Q10%, adjusted for age, sex, socioeconomic status and comorbidity. The positive standardized β coefficients for all diseases denote influence of therapy on HRQoL even when adjusted. For many diseases the β coefficient was relatively high, indicating robustness of the presented results.
Table II. Effect of treatment on Dermatology Life Quality Index (DLQI). Ranking according to the percentage of Question 10 of the DLQI (therapy issues) to the mean total DLQI (Q10%) for diagnoses with at least 20 valid answers (hyperhidrosis (12), nail diseases (17) and granuloma annulare (13) excluded). Linear regression (standardized β) with “naevi” as a “healthy” control group, adjusting for age, sex, socioeconomic status and comorbidity (diabetes mellitus, cardiological, respiratory, rheumatological or other disease)
When assessing Q10%, males and older patients showed more impairment, the reverse of what was seen for total mean DLQI. The impairment was highest in patients with comorbidities or those of low socioeconomic status.
When considering the impact of therapy on HRQoL, highest mean scores and most positive answers to question 10 were seen in diseases that commonly affect large areas of the skin (e.g. AD, psoriasis, allergic/drug/phototoxic conditions, prurigo, papulosquamous diseases, eczemas, connective tissue disease and vitiligo), as well as diseases accompanied by blisters/erosions, ulceration or crusting (blistering diseases, venous leg ulcer, vasculitis, immunological ulcers and oral diseases) and pruritic dermatoses (prurigo, urticaria and pruritus) (Table II, Fig. 1).
Q10% reveals which diagnostic groups are most affected by therapy relative to their total HRQoL impairment. Blistering conditions showed the highest value (10.7), followed by allergic, drug, phototoxic/-allergic reactions (10.2) and psoriasis (9.9), a ranking that differs from total mean DLQI values (Table SII). This gives insight into the true extra burden of therapy for different diseases.
HS, prurigo, pruritus and urticaria show the highest impairment when mean DLQI scores are evaluated, but drop in ranking when therapy is assessed. Likewise, acne, rosacea and psychodermatological conditions, scoring among the average impaired as measured by mean DLQI scores, were some of the least affected by therapy. Conversely, blistering conditions, non-melanoma skin cancer (NMSC), actinic keratoses (AK), allergic/drug reactions, vasculitis and venous leg ulcers rank higher when evaluated according to therapy-related impairment.
Using a dermatology-specific measure this study identified the extent of the reduced HRQoL associated with therapy. For several diseases, patients experience a high burden associated with therapy (blistering conditions, allergic/drug reactions, psoriasis, vasculitis, vitiligo and venous leg ulcers). Ranking the diseases according to what percentage of the burden is caused by therapy gives new insight into this specific impairment for the separate diagnoses.
Most skin diseases are treated with topical therapy. However, dermatological treatments include oral therapy, phototherapy, photodynamic therapy, lasers, cryotherapy, intralesional and surgical procedures and parenteral administrations, which may be painful, time-consuming or cause infusion reactions. The use of these specific dermatological medications and therapeutic approaches presents issues and challenges unique to skin disease.
Generic HRQoL measures have been developed without specific reference to the impact of therapy for skin disease (Table III). Assessment may therefore be inaccurate if this burden experienced by dermatological patients is missed. There are no questions related to the impact of therapy in the most commonly used generic measures. However, the generic measures Treatment Satisfaction with Medicines Questionnaire (SATMED-Q) (3) and Treatment Satisfaction Questionnaire for Medication (TSQM) (4) are designed to address issues with medication, but are little used in dermatology. The DLQI is the only non-disease-specific dermatological measure that addresses therapy burden (Table III), although the DLQI is the most widely used measure in dermatology (14) the issue of therapy is little explored.
Table III. Overview of dermatology-specific, disease-specific and generic instruments assessing quality of life with comments on whether the impact of therapy is addressed in the questionnaire
There are very few studies evaluating the contribution of therapy to impairment of HRQoL. In 3 studies (15–17) the generic instrument Short Form Health Survey (SF-36) was used in random samples of the population. A large proportion of patients reported dermatological problems and those using topical therapies on prescription showed greater impairment of HRQoL than those not using topical prescription medicines (15). An overview of the most relevant results for several diagnoses is given below.
Blistering diseases showed the highest impairment due to therapy and positive standardized β values as high as 0.5, in support of the high impairment caused by the disease and its therapy and not because of the age, sex, comorbidity or socioeconomic status of the patients.
HS results in severely impaired HRQoL (18, 19), has the highest mean DLQI, but scores for Q10% are low. Studies of the same data-set rank HS patients with some of the lowest HRQoL (8), highest risk for psychiatric comorbidity (7, 20) and impairment in sexual life (9). Despite very high impairment of HRQoL, therapy contributes little to this burden.
AD and psoriasis rank highly when mean DLQI, positive answers to therapy issues or Q10% are evaluated, suggesting that these patients are equally adversely affected by all aspects of HRQoL, including therapy.
Diseases affecting small areas of the body, such as facial dermatoses (seborrhoeic dermatitis, rosacea and acne), as well as psychodermatological conditions rank lower on therapy relative to the total DLQI than might be expected, demonstrating that it is the disease itself and not the therapy that is the driving cause of HRQoL impairment. Treating these conditions adequately should alleviate the patient’s experienced burden without additional impairment.
In contrast, patients with AK, NMSC, allergic/drug reactions, scars/fibrosis and morphea, who do not report severe impairment of HRQoL as measured by the mean DLQI, rank highly in impairment when assessing therapy as a percentage of this total score. AK and NMSC do not apparently have a high impact on HRQoL, nor psychiatric comorbidity (7, 8, 20), but score relatively worse when therapy is assessed, ranking them higher than HS and several other diseases.
Studies evaluating the burden caused by AK and/or NMSC have shown low impact on HRQoL of these diseases (21–24), raising the possibility that currently available measures may be missing therapy issues and that there may be a need for a skin-cancer-specific HRQoL measure. Existing disease-specific instruments do not include therapy questions (22, 25) (Table III).
Burdensome treatments have a negative effect on adherence to therapy (5) and can be the reason for undertreatment and relapse of disease. Measuring HRQoL without taking into account therapy issues may not represent the true extent of suffering that dermatological patients experience. On the other hand, knowing which diseases have the highest potential to cause therapy issues can alert clinicians to which patients need a different approach, by giving them better information, providing a variety of options, offering training in therapy application, or at least acknowledging the issue.
When developing clinical guidelines in dermatology, optimization of therapy and minimizing the burden of treatment should be considered. Developers of HRQoL instruments should pay attention to therapy issues when measuring HRQoL in some specific diagnoses, such as skin cancer, as this burden may go undetected using currently available measures (7, 8, 20–23).
The high number of patients in this study, the unbiased selection of participants and adjusting for confounding factors resulted in robust data on therapy as a factor contributing to impairment in HRQoL. Similar studies on therapeutic issues are lacking and studies using DLQI typically have no healthy control group.
One potential limitation is in the detail of the wording of DLQI question 10: “(…by making your home messy, or by taking up time)”, which may bias the respondents into only considering topical therapy. However, the main question itself is neutral on this point “…how much of a problem has the treatment for your skin been…”.
Detailed information on all treatments used by our patients was not obtained systematically. The presented data evaluate therapy issues on a general basis. Further studies evaluating specific dermatological treatments are warranted.
Although we refer to data from each country, the data was based on 1 centre from each country (apart from Italy and Norway). The recruitment centres may not have been representative of clinical practice across each country. There were large differences between countries in scores assessing impairment, which cannot be readily explained. The cross-cultural issue is one that is of relevance to all HRQoL measures (26). The same limitation may apply when comparing diseases (27). The cultural and language factors leading to these differences are not fully understood, though they should be taken into account when making any cross-cultural comparisons and when using HRQoL data as a guide to optimal health policies and creating optimal treatment guidelines. Analysis of the source for country differences may be able to serve as a guide to optimal health policies and creating optimal treatment guidelines.
Treatments for skin diseases contribute to the burden on HRQoL. For some diagnoses, therapy may have a larger impact than was previously known, but we also identify diseases that are affected by therapy to a lesser degree. Older, male patients with lower socioeconomic status and comorbidities experience more adverse issues with therapy. This study highlights new aspects to HRQoL that may have previously been overlooked. Clinicians are made aware of the importance in addressing therapy issues and promoting adherence to therapy, and pharmaceutical companies of the ease of use of their products. Developers of HRQoL instruments should consider including therapy-related questions. The ultimate goal would be to reduce the burden of skin disease and promote adherence to therapy.
The European Society for Dermatology and Psychiatry (ESDaP) initiated the study. The authors thank the ESDaP Group who collected and validated the data and Geir Strandenæs Larsen who helped with data search.
AYF is joint copyright owner of the DLQI. Cardiff University and AYF receive royalties (though not from this study). The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize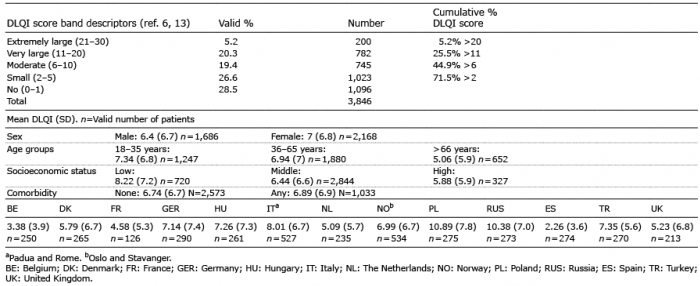 Click to show fullsize
Click to show fullsize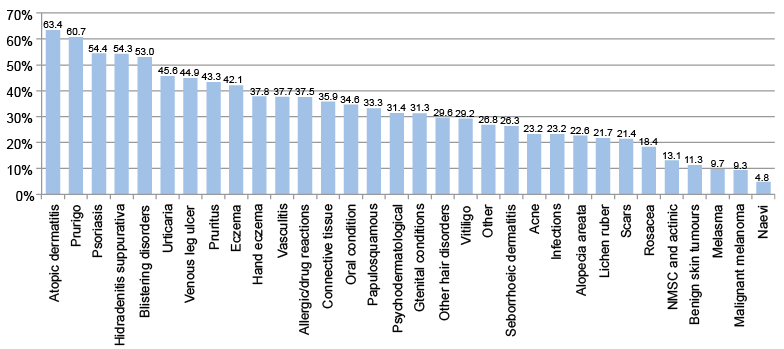 Click to show fullsize
Click to show fullsize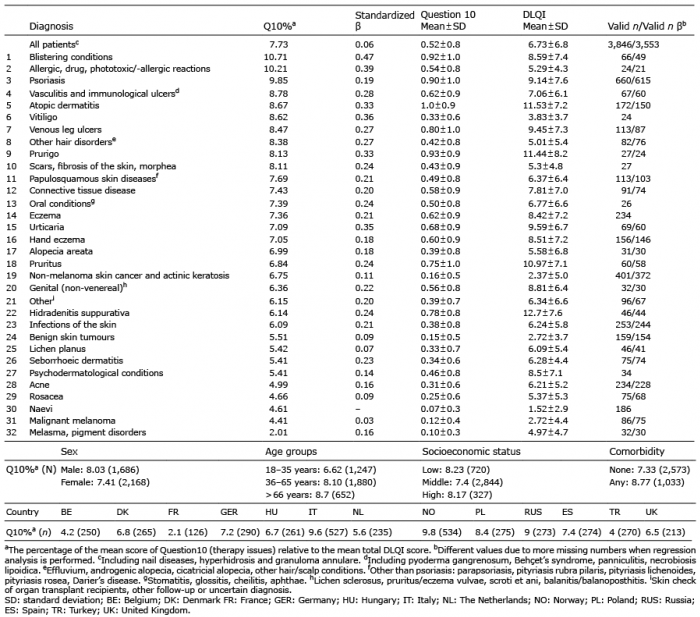 Click to show fullsize
Click to show fullsize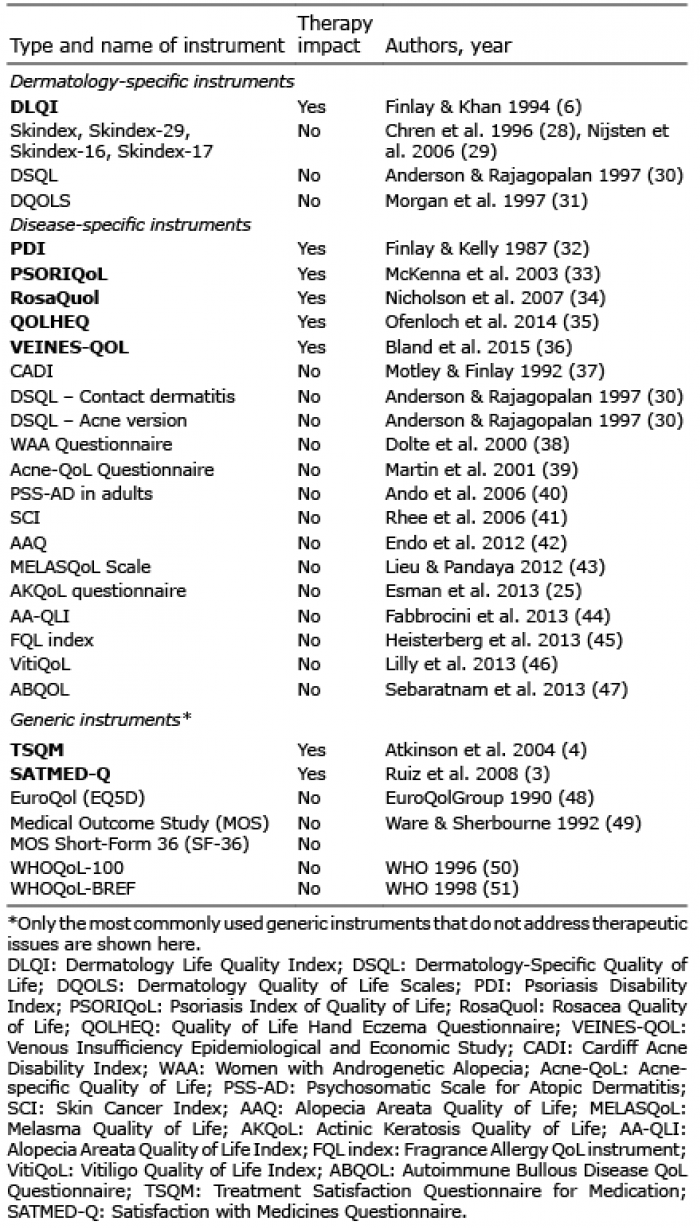 Click to show fullsize
Click to show fullsize