


1Department of Adult Psychiatry and Medical Psychology, Clermont-Ferrand University Hospital, Clermont Auvergne University, 2Department of Adult Psychiatry and Medical Psychology, 3Department of Clinical Research and Innovation and 4Department of Dermatology, Clermont-Ferrand University Hospital, Clermont Auvergne University, Clermont-Ferrand, and 5Paris Descartes University, Sorbonne Paris Cité, Faculty of Medicine, Paris, France; AP-HP, West Paris University Hospitals, Department of Psychiatry, Paris, France
#These authors contributed equally to this work.
Impaired emotional abilities (higher scores of alexi-thymia and lower levels of emotional awareness) were found in patients with skin-restricted lupus, warranting examination of the relationship between these abilities and the evolution of skin-restricted lupus, using longitudinal data. A total of 75 consecutive outpatients with skin-restricted lupus were recruited and assessed by a dermatologist and a psychiatrist every 6 months over a period of 2.5 years. Alexithymia and emotional awareness were evaluated with the French versions of the Toronto Alexithymia Scale (TAS-20) and the Levels of Emotional Awareness Scale (LEAS). During follow-up, good stability of the LEAS scores was observed, whereas TAS-20 scores varied; those variations were positively associated both with lupus duration and current psychiatric and personality disorders, but not with lupus remission. Such findings regarding 2 complementary aspects of emotional functioning are of direct interest for the management of patients with skin-restricted lupus.
Key words: skin-restricted lupus; alexithymia (TAS-20); Levels of Emotional Awareness Scale (LEAS); psychiatric disorders; longitudinal study; emotional processing.
Accepted Mar 4, 2019; E-published Mar 5, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Isabelle Jalenques, Department of Adult Psychiatry and Medical Psychology, Clermont-Ferrand University Hospital, Clermont Auvergne University, 58 rue Montalembert, FR-63003 Clermont-Ferrand Cedex 1, France. E-mail: ijalenques@chu-clermontferrand.fr
Patients with skin-restricted lupus (SRL) have impaired emotional abilities, i.e. higher alexithymia (inability to identify and describe emotions) and lower emotional aware-ness. This follow-up study investigated the relationship between emotional abilities and the evolution of SRL. The results showed no direct relationship between SRL remission and emotional abilities. Good stability of emotional awareness scores was observed, whereas alexithymia scores varied; these variations were positively associated both with duration of lupus and the presence of current psychiatric and personality disorders. Such findings are of direct interest for the management of patients with SRL.
Psychiatric and personality disorders have been reported recently among patients with skin-restricted lupus (SRL) i.e. discoid lupus erythematosus (DLE), lupus tumidus (LT) and subacute cutaneous lupus erythematosus (SCLE) (1–4), as reported among patients with systemic lupus erythematosus (SLE) or some chronic inflammatory skin diseases (5–10).
Impaired emotional abilities have also been described: alexithymia, a difficulty in recognizing and communicating emotions, has been reported in SLE (11–15) and skin diseases (16–21); and lower emotional awareness (the capacity to represent, discriminate and elaborate both one’s own and others’ emotional experience in a given context) has been reported in patients with psoriasis who consider their disease to be stress reactive (18). We recently demonstrated, in a case-control study, that patients with SRL had impaired emotional abilities (22), i.e. exhibited higher alexithymia scores and lower emotional awareness levels, than controls. Alexithymia scores, but not emotional awareness levels, were associated with concurrent psychiatric or personality disorders in patients with SRL: the case-control differences persisted after adjusting for such disorders, for emotional awareness levels, but not for alexithymia scores.
In SLE, no significant correlation was observed between alexithymia and medical variables, in contrast to psychopathological symptoms, especially depression and anxiety (11, 13). In psoriasis, one study reported that alexithymia was associated with higher disease burden, including significant impairment of quality of life, higher levels of anxiety and depression, a higher risk of alcohol dependency and impairment of work productivity (19), while another did not find any association between alexithymia and psoriasis severity, but higher scores of alexithymia in the case of involvement of sensitive areas, such as the face, hands, and genital area (20). In addition, lower levels of emotional awareness predicted a better response to dermatological treatment in psoriasis (18).
Given that our case-control study on SRL encompassed a longitudinal, prospective component, we decided to explore the relationship between emotional abilities and evolution of SRL. The objectives of this study were to assess, over a 2.5-year period: (i) SRL remission according to baseline alexithymia and emotional awareness scores; and (ii) the changes in alexithymia and emotional awareness scores and the factors associated with such changes.
The study received approval from the local ethics review board (Comité de Protection des Personnes Sud-Est 6, reference 2008-A00343-52 / AU740, 18 June 2009). The aims and procedures were explained to participants, who all gave written informed consent.
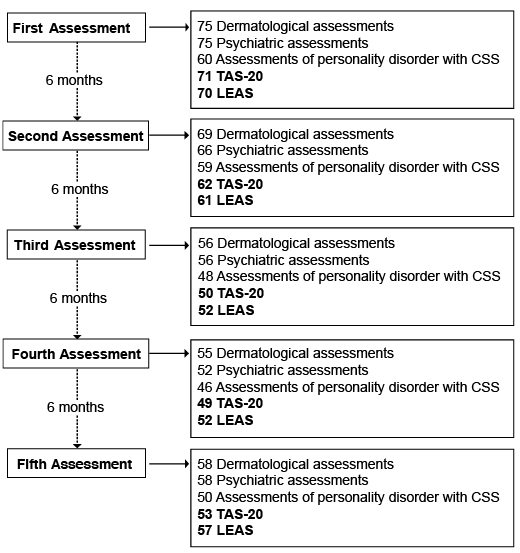
Eighty consecutive outpatients with chronic SRL (DLE and LT) or SCLE were recruited from 8 French university hospitals. Inclusion criteria are shown in Table SI. They were assessed by a dermatologist and a psychiatrist every 6 months for a period of 2.5 years (Fig. 1).
Fig. 1. Flow chart of the number of patients evaluated during the follow-up for each assessment/scale. CSS: Clinical Significance Scale; TAS-20: Toronto Alexithymia Scale; LEAS: Levels of Emotional Awareness Scale.
The dermatologist determined whether the cutaneous lupus was in complete remission, as defined by the absence of any inflammatory lesions. Lupus history comprised the date of first symptoms, ongoing and past specific treatments, and smoking habits.
A psychiatrist assessed the presence of current Axis I psychiatric disorders using the Mini International Neuropsychiatric Interview (MINI 5.0.0) (23, 24). Personality disorders were investigated by the latest version of the self-report Personality Diagnostic Questionnaire 4+ (PDQ-4+): when a personality disorder is suggested, according to the PDQ-4+ cut-off points, the psychiatrist has to confirm or rule out this diagnosis on the basis of the clinical significance scale of the PDQ-4+ (CSS) (25–27). More details of the means of assessment can be found in our previous articles on psychiatric and personality disorders in patients with SRL (2, 4).
Alexithymia and emotional awareness were evaluated with the French versions of the Toronto Alexithymia Scale (TAS-20) and the Levels of Emotional Awareness Scale (LEAS), which have been suggested to be used simultaneously (28). The TAS-20, the most widely used measure of alexithymia to date, is a self-report questionnaire consisting of 20 statements. Subjects assess their agreement or disagreement with the statement on a 5-point Likert scale. The total alexithymia score is the sum of the responses to all 20 items (range 20–100) (29).
The LEAS is a performance instrument that asks the subject to write down his or her anticipated feelings and those of another person for each of 20 different standard scenarios. The scenarios are described in 2–4 sentences and involve 2 people, followed by 2 questions (“How would you feel?” and “How would the other person feel?”). The scenarios aim to evoke 4 types of emotion: anger, fear, happiness and sadness (30), but all scenarios are scored in the same way. The score for each scenario ranges from 0 to 5 (from no answer or non-emotion responses to multiple blends of differentiated emotions attributed to self and others that are non-identical). Scores were computed according to a glossary of words and phrases (31). The total LEAS score is the sum of the scores for the 20 items, with the maximum possible total score being 100. All the LEAS protocols were rated blind to psychiatric status and to the order of the follow-up evaluation, as in previous studies with a similar design (32).
Statistics were computed with STATA V12 (Stata Corp, College Station, TX, USA).
TAS20 and LEAS baseline scores were compared between groups (no remission vs. remission at any time during follow-up) using Students t-test (or Mann–Whitney test when data were not normal).
Stability of TAS20 and LEAS scores during follow-up were analysed using intraclass correlation coefficient (ICC). A longitudinal linear mixed model was computed, taking the patient as random effect and the follow-up visit as fixed effect.
The longitudinal analysis of factors associated with TAS-20 score changes during the follow-up was performed using multiple generalized linear regression mixed models, taking the patient as the random effect and adjusting for fixed effects, as the follow-up visit, and factors that were clinically relevant. The results are shown as regression coefficient estimates and their 95% confidence interval (CI).
All tests were 2-sided and a p-value < 0.05 was considered statistically significant.
The baseline characteristics of the 75 participants for whom we had complete dermatological data are described in Table I. Briefly, patients were predominantly women (80%) and smokers (59%), mean age was 46.2 ± 13.4 years, age at first lupus symptoms was 36.3 ± 14.3 years, and mean duration of disease was 10.2 ± 7.5 years; 55 (74%) patients had chronic lupus and 19 (26%) a subacute form. Fifty-three patients (72%) had lesions on a visible area of the body. Fifty-nine patients (80%) were receiving treatment for lupus and 21 (28%) a psychotropic medication, whereas 37 patients (49%) had a current psychiatric disorder and 23 (38%) had a personality disorder. Twenty-two (29%) patients had analgesic medication, mainly paracetamol for headache, tendonitis, hernia, and sciatica. With respect to comorbidities, 15 patients (20%) had a cardiovascular disease, 13 (17%) diseases of the digestive system, 7 (9%) diseases of the genitourinary system, 6 (8%) an endocrine, nutritional or metabolic disease and 6 (8%) diseases of the osteo-articular system, muscles and connective tissue. Baseline TAS-20 and total LEAS scores are shown in Table I. They were related neither to analgesic medication nor to medical comorbidities (data not shown).
Table I. Baseline patients’ description
Although some patients have not completed all follow-up assessments (Fig. 1), they had 4 assessments, on average; and we have verified that there was no difference in patient participation in the study according to the TAS-20 and LEAS baseline scores (Spearman’s correlation coefficient r = –0.05, p = 0.65 and r = 0.17, p = 0.16, respectively).
First, we investigated if baseline TAS-20 and LEAS scores were associated with remission of SRL. Both baseline TAS-20 and LEAS scores did not differ between the 33 patients who were never in remission and the 38 patients who were in remission at any time during the follow-up (48.0 ± 11.1 vs. 49.2 ± 11.3, p = 0.67 and 48.6 ± 12.7 vs. 49.6 ± 10.9, p = 0.72, respectively).
Evolution of the TAS-20 and LEAS scores in patients with SRL during the follow-up was then assessed. Although the distribution of TAS-20 and LEAS scores showed good stability over time (Fig. 2), we checked that there was no intra-individual variation with an intraclass correlation analysis. While the intraclass correlation was good for LEAS (ICC 0.80 [0.75–0.86]), proving a good stability of LEAS score, it was not for TAS-20 (ICC 0.56 [0.47–0.66]).
Fig. 2. Toronto Alexithymia Scale (TAS-20) and Levels of Emotional Awareness Scale (LEAS) score distributions during the follow-up. Box plots (median, interquartile range and 95% confidence interval) representing TAS-20 and Total LEAS scores of patients during the 5 follow-up assessments. Cross=mean score; circle=extreme values.
As TAS-20 scores varied during follow-up, we looked for dermatological or psychological factors that could affect the score (Table SII). Thus, the effects of tobacco consumption, lupus duration, lupus remission, personality or psychiatric disorders at any assessment, and the effect of the different follow-up assessments were analysed on TAS-20 scores. Current personality or psychiatric disorders and lupus duration were associated with higher TAS-20 score (Table II). Remission or not of lupus did not change the TAS-20 score in any way.
Table II. Factors affecting Toronto Alexithymia Scale (TAS-20) score over 2.5 years of follow-up
This study reports, for the first time, 2 complementary aspects of emotional ability during the evolution of SRL; alexithymia and emotional awareness.
The study population was similar to skin lupus populations described elsewhere in terms of male-female ratio (20/80) and age at lupus onset (33) and none of the cases in the current study has evolved towards systemic lupus during a median follow-up of 43 months. The majority of patients completed all follow-up assessments.
Alexithymia is a major facet of emotion processing impairment, usually measured by the TAS (34). Our study shows that TAS-20 scores varied during the follow-up; those variations were associated both with SRL duration and current psychiatric and personality disorders. The association with lupus duration could be likened to a previous publication in which we reported that lupus duration was an associated risk factor for current psychiatric disorders in patients with SRL (2). In other inflammatory diseases, few studies have investigated whether there was an association between alexithymia scores and evolution of the diseases (18, 35). The current results demonstrated that the TAS-20 scores were not associated with SRL remission, as in psoriasis and inflammatory bowel disease (18, 35), in the same way that the baseline TAS-20 score was not related to the severity of dermatological lesions.
In the previously reported cross-sectional data in our case control study, TAS-20 scores in patients with SRL were positively associated with current psychiatric and personality disorders (22). Analysis of longitudinal prospective data showed that TAS-20 scores also varied according to current psychiatric and personality disorders. Even though alexithymia can occur among medically ill patients without psychiatric comorbidity (36), an association between alexithymia and depression or anxiety has been reported in the general population (37) and among patients with SLE (13–15); moreover, an association between alexithymia and certain personality dimensions, notably “neuroticism”, has been observed in patients with SLE (13). However, to our knowledge, no study has examined variation in alexithymia during the follow-up of patients with SLE or those with chronic inflammatory skin disease. In addition, Sampogna et al. highlighted the interest in conducting a study in psoriasis to determine whether alexithymia is stable over time and whether treatment impacts on alexithymia (38). One study has reported that alexithymia is stable over time in the general population and acts as a personality trait (39), which confirmed the data of Luminet et al. (40). The latter proved that, in outpatients with major depression, alexithymia scores changed with changes in depression scores, indicating a lack of absolute stability, but that differences among individuals remained the same over time and that alexithymia scores at baseline correlated significantly with alexithymia scores at follow-up, even after adjusting for depression severity, indicating a relative stability of alexithymia (40). Our 2.5-year follow-up results indicate, for the first time, that both the duration of a burdening medical condition and the presence of a psychopathology (both being associated) can be associated with alexithymia. These data support the hypothesis of a “secondary” alexithymia, associated with or induced by psychiatric or personality disorders, in patients with medical illnesses, in addition to a “primary”’ alexithymia, not exclusively associated with such disorders, which could act as a risk factor for various somatic morbidities through less effective defences against stress (32, 36).
The construct of levels of emotional awareness offers an alternative way of measuring emotional abilities (41). In 3 previous publications on case-control comparisons, LEAS was a more robust tool for assessing emotional ability than TAS-20, in the presence of psychiatric comorbidities or personality disorders (22, 32, 42). During follow-up, we also observed good stability of the LEAS scores. This difference could be partly explained by the fact that TAS-20 scores are based on self-assessments, and so can be influenced by the level of distress of respondents, whereas the LEAS does not involve self-rating and is not influenced by self-reported distress (32, 41, 43). In addition, TAS-20 and LEAS measure different aspects of emotional functioning (43).
Patients with SRL with impaired emotional abilities represent a high-need subgroup of patients. Indeed, although our study does not show any link between alexithymia or impaired emotional awareness and SRL activity, relationships between alexithymia and poor compliance with medical treatment have been documented (44, 45), In addition, our study shows that alexithymia can be associated with psychiatric disorders, which are highly prevalent in patients with SRL (2). Such disorders should therefore be screened for, in order to offer suitable additional treatment if needed, especially as it has been demonstrated that psychotropic drugs help in achieving remission of SRL in patients with psychiatric disorders (46). Three hypotheses could be considered with regard to the underlying mechanisms: first, less-depressed patients may be more compliant with their dermatological treatment; secondly, if the SRL has a psychosomatic component, the less-depressed patients may be less responsive to stress and their dermatological disease more stable; and thirdly, antidepressants with anti-inflammatory properties may have an independent or additional effect on SRL (47). A dermatologist is often a central caregiver for patients with SRL; in such cases, the medical consultation is an excellent opportunity to discuss the psychological state of the patient. Clinicians should not hesitate to refer such patients for specialized mental health evaluation and care: if low emotional awareness and less effective stress management strategies are identified, appropriate psychotherapy could be offered (48, 49).
The current study presents certain limitations. First, it did not use an observer-rated interview for assessing alexithymia, but a self-administered questionnaire, the TAS-20, with the possibility of false-negative and false-positive results. However, the study was greatly enhanced by having combined 2 complementary measures of emotion processing, the TAS-20 and the LEAS, and assessments of depression, anxiety and other psychiatric disorders, a multi-method approach whose value has already been attested to (32, 43). Secondly, it is not known whether the patients with alexithymia or low emotional awareness underwent the same therapeutic compliance during the 2.5 years of their lupus treatment. However, there was no difference in participation throughout the study according to the TAS-20 and LEAS scores at baseline. In addition, it is not known whether the patients with SRL were engaged in psychotherapy during their medical follow-up. Thirdly, because of its design, the study does not indicate whether patients were already characterized by lower emotional abilities before their SRL was established. It can be speculated that the burden of disease and the occurrence of a psychopathology could have increased the alexithymia, since the latter is positively correlated both with the duration of SRL and psychopathology.
The results of this longitudinal study, combined with data from the previous publication (22), provides evidence for the first time of 2 complementary aspects of emotional functioning during the evolution of SRL. The previous publication showed first that patients with SRL have higher alexithymia and lower emotional aware-ness scores and, second, that only alexithymia is both positively associated with lupus duration and current psychiatric and personality disorders. This longitudinal study shows that alexithymia increases during follow-up in case of psychiatric disorders, whereas the emotional awareness of the patients is not affected in case of such disorders; thus, patients with SRL with a level of emotional awareness lower than the controls keep their level lower throughout the evolution of SRL. In addition, these results indicate that the measure of emotional abilities should not be limited by use of the TAS alone, since the latter is very much influenced by psychiatric disorders, while LEAS proved a more robust tool for emotional ability evaluation and could therefore be used in further studies to examine the association of impaired emotional awareness with inflammation status or minimal brain damage in patients with SRL.
This study was supported by a grant from the French Ministry of Health (PHRC IR 2006 Jalenques, N°2008-A00343-52) and from Société Française de Dermatologie, 2010.
The LuPsy cohort investigators: François Aubin (Franche Comté University, Besançon University Hospital, Department of Dermatology, Besançon, France ), Christophe Bedane (Department of Dermatology, Hopital Dupuytren, Limoges, France), Sophie Bonnefond (Department of Psychiatric Emergencies, Esquirol Hospital, Limoges, France), Myriam Chastaing (Department of Liaison Psychiatry and Department of Dermatology, Brest University Hospital, Brest, France), Marianne Collange (Department of Adult Psychiatry and Medical Psychology, Clermont-Ferrand University Hospital, Clermont-Ferrand, France), Patrick Combemale, Denys Courbier (Desgenettes Army Training Hospital, Lyon, France), Carole Durand (Department of Adult Psychiatry and Medical Psychology, Clermont-Ferrand University Hospital, Clermont-Ferrand, France), Jean Paul Grand (Le Valmont Hospital, Emergencies and Liaison Psychiatry, Valence General Hospital, Valence, France), Emmanuel Haffen (Department of Clinical Psychiatry, INSERM, University Hospital of Besançon, Besançon, France ), Bruno Labeille (Department of Dermatology, Nord University Hospital, Saint-Etienne, France), Catherine Massoubre (Department of Psychiatry, St-Etienne University Hospital, University Jean Monnet, St-Etienne, France), Laurent Misery (University Hospital of Brest, Department of Dermatology and University of Western Brittany, Laboratory of Neurosciences of Brest, Brest, France), Jean-Luc Perrot (Department of Dermatology, Nord University Hospital, Saint-Etienne, France), Anne Laure Pontonnier (Department of Adult Psychiatry and Medical Psychology, Clermont-Ferrand University Hospital, Clermont-Ferrand, France), Robert Schwan (University Hospital of Psychiatry and Psychotherapy, Laxou, France), François Skowron (Department of Dermatology, Valence Hospital, Valence, France), Agnès Sparsa (Department of Internal Medicine, Clinic Mutualiste Catalane, Perpignan, France), Gaëlle Theilhol (Department of Adult Psychiatry and Medical Psychology, Clermont-Ferrand University Hospital, Clermont-Ferrand, France), Julie Waton (Department of Dermatology, Nancy University Hospital, Nancy, France).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize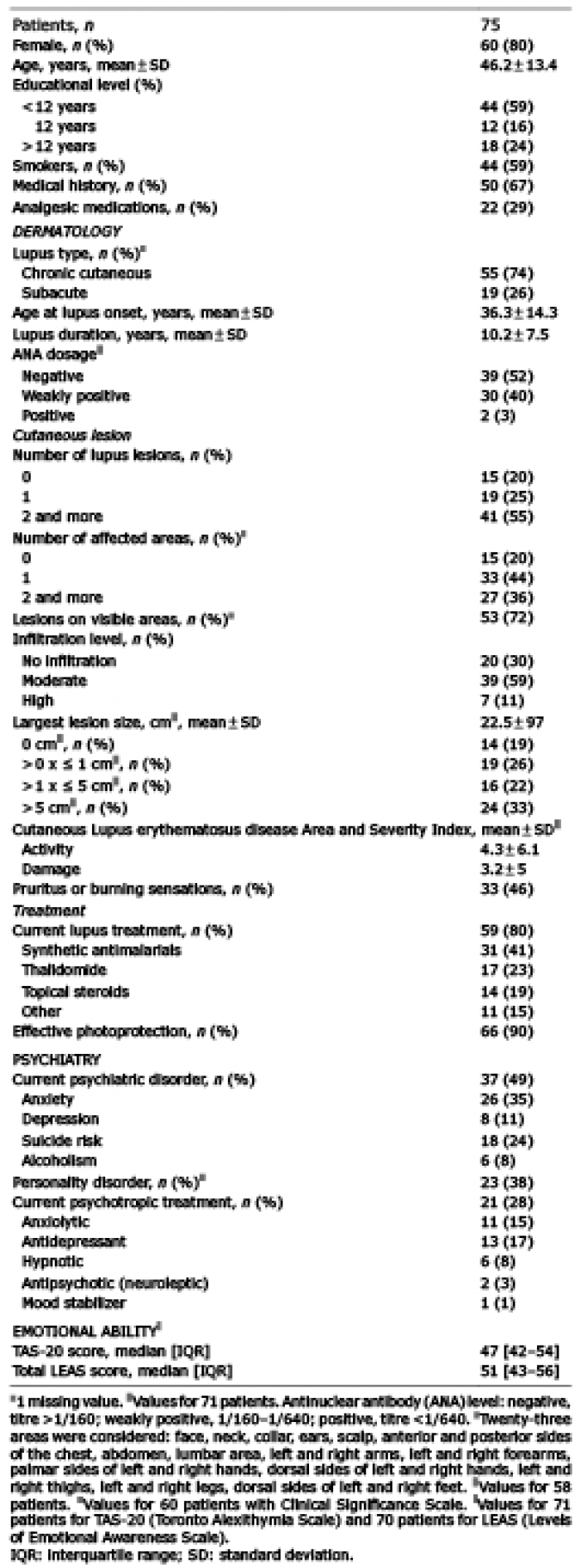 Click to show fullsize
Click to show fullsize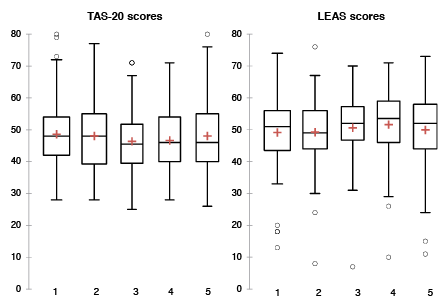 Click to show fullsize
Click to show fullsize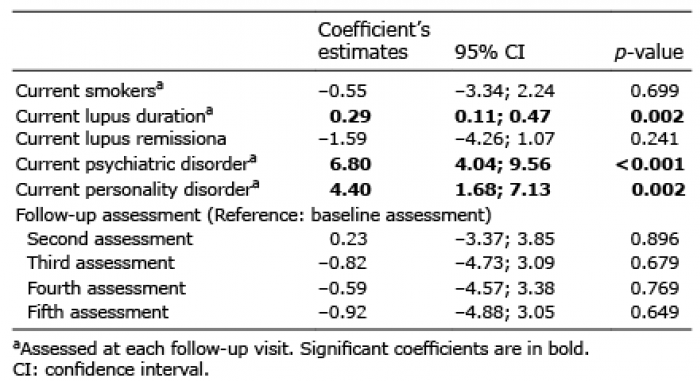 Click to show fullsize
Click to show fullsize