


Johanna Braegelmann1, Angelo Massimiliano D’Erme1,2, Sidikov Akmal3, Judith Maier1, Christine Braegelmann1 and Joerg Wenzel1*
1Department of Dermatology and Allergy, University Hospital of Bonn, Sigmund-Freud-Strasse 25 DE-53127 Bonn, Germany, 2Unit of Dermatology, University of Pisa, Pisa, Italy, and 3Department of Dermatovenereology, Saint Petersburg State Pediatric Medical University, Saint Petersburg, Russia. *E-mail: joerg.wenzel@ukb.uni-bonn.de
Accepted Oct 29, 2015; Epub ahead of print Nov 2, 2015
Erythroderma is an acute and serious medical condition characterized by inflamed red skin affecting over 90% of the skin surface. Palmoplantar involvement with hyperkeratosis and fissuring is common. A serious and potentially life-threatening complication is the loss of fluid and albumin through the eroded skin, leading to displacement of electrolytes. As a result, patients become dehydrated and hypothermic.
Psoriasis vulgaris, eczema, cutaneous T-cell lymphoma (CTCL) and drug reactions are the most common underlying causes of erythroderma (1, 2). Despite their differing pathomechanisms, clinical diagnosis of erythroderma cases can be problematic. The criteria for histological examination cannot be defined precisely at any stage of the disease (1, 2). Exact diagnosis of the underlying disease is, however, of great importance for patients, due to the considerable differences between the therapeutic regimes.
We have recently found that interleukin (IL)-36γ, an IL-1-family member, is expressed specifically in the epidermis of psoriasis vulgaris patients and thus is a reliable marker in distinguishing psoriasis from other erythematosquamous skin diseases, including atopic dermatitis and lichen planus (3).
The aim of this study was to investigate the usefulness of immunohistological IL-36γ staining in the diagnosis of psoriasis-based erythroderma among erythrodermic cases.
PATIENTS AND METHODS
All skin samples were taken from the archives of the Department of Dermatology and Allergy, University Hospital Bonn. Only biopsies that were sent in between 2001 and 2011 with the clinical diagnosis “erythroderma” were included (n = 46). The final diagnosis was retrospectively taken from the patients’ files. The follow-up period lasted between 3 and 13 years. The study was performed in accordance with the principles of the Declaration of Helsinki. Sections were prepared from formalin-fixed, paraffin-embedded skin biopsies. Standard haematoxylin and eosin (H&E) as well as periodic acid–Schiff staining have been performed for diagnostic purposes. Protein expression of IL-36γ was analysed by immunohistochemistry using a monoclonal mouse immunoglobulin G1 (IgG1) anti-human-IL-36γ antibody (ab156783, Abcam, Cambridge, MA, USA; dilution 1:500). Visualization was achieved using the REAL staining kit (DAKO, Hamburg, Germany) with Fast Red as chromogen (3).
H&E sections were scored on the basis of established histological criteria (0 = none, 1 = weak, 2 = fair, 3 = strong) in order to distinguish between the underlying diseases (4). These histological criteria included hyper-/parakeratosis, hypogranulosis, akanthosis, spongiosis, hydropic degeneration, “lining”, lymphocyte microabscesses, epidermal neutrophilic infiltrate, pear-like acanthosis, expanded rete ridges, dermal eosinophilic infiltrate and dermal neutrophilic infiltrate (1, 2, 5, 6). IL-36γ-expression was counted by positive cell layers (≤ 1, 2–3, ≥ 4) in a blinded fashion, as described previously (3). Statistical analyses were done by SPSS 23 using the non-parametric Mann-Whitney U test.
RESULTS
Eleven of the erythrodermic patients had eczema, 12 psoriasis, 9 drug reactions and 8 CTCL. In one case the underlying disease could be identified as pityriasis rubra pilaris (PRP), one other patient had graft-versus-host-disease (GvHD) and in 4 cases the cause of erythroderma could not be identified clearly (unclear). These latter 6 patients were merged to the category “others” (Table SI1).
The morphological scoring of our skin samples revealed a typical, but not specific, morphological pattern for all common underlying diseases. Psoriasis samples showed hyperparakeratosis, hypogranulosis, pear-like acanthosis and elongated rete ridges. Neutrophils were present in the epidermis (stratum corneum) and dermis. However, none of these morphological criteria alone was able to identify psoriasis patients: in eczema (and to a lower degree in CTCL), hyperparakeratosis and acanthosis were also common, and, to a lesser extent, hypogranulosis, pear-like acanthosis and expanded rete ridges (the latter also in CTCL).
Importantly, a specific affection of the basal epidermis with a lymphocytic infiltrate (hydropic degeneration, lining of lymphocytes along the basal membrane or lymphocytic microabscesses) was seen only in CTCL and drug reactions. These features are exclusion criteria for psoriasis, but are also absent in eczema (detailed data is given in Table SI1 and SII1).
Among the different underlying diseases, patients who had psoriasis showed significantly enhanced mean expression of IL-36γ within their skin lesions (Fig. 1a). None of the psoriasis patients had a lesional IL-36γ-expression ≤ 1 cell layer and an expression of ≥ 4 cell layers was only seen in psoriasis (Fig. 1b). Representative histological micrographs are shown in Fig. 1c–f.
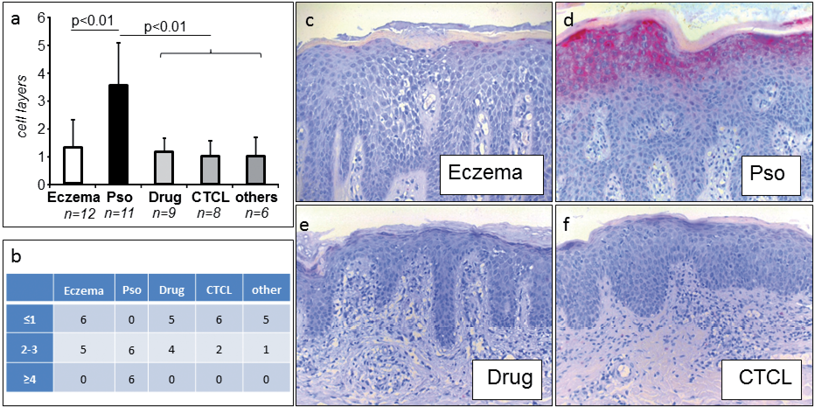
Fig. 1. Interleukin (IL)36γ expression in different erythroderma subsets. (a) Number of IL-36γ-positive cell layers detected by immunohistochemistry in the different disease subsets (mean expression ± standard error of the mean (SEM)). (b) Number of specimens with low (0–1 cell layers), fair (2–3 cell layers) and strong (≥ 4 cell layers) expression of IL-36γ within the different subsets. (c–f) Representative IL-36γ-micrographs (eczema, psoriasis (Pso), drug-reaction and cutaneous T-cell lymphoma (CTCL), original magnification × 200, respectively).
DISCUSSION
IL-36γ, formerly known as IL-1F9, is a member of the IL-1 family. The IL-36 family comprises the agonistic cytokines IL-36α (= IL-1F6), β (= IL1F8) and γ (= IL-1F9) as well as the antagonistic cytokine IL-36Ra (= IL-1F5), which are involved in the regulation of innate as well as adaptive immune responses (7, 8). Importantly, patients with a genetic loss of the IL36-inhibitor IL36-RN experience severe pustular-psoriasis-like skin lesions, directly connecting the IL36-cytokines with this disease (9).
We have shown recently that IL-36γ is a specific biomarker of psoriasis vulgaris. This cytokine is specifically expressed in psoriasis skin lesions, and IL36γ-serum levels are closely associated with psoriasis disease activity (3). IL-36γ induces the production of psoriasis-typical cytokines, including IL-12, IL-23 and TNFα. It contributes to skin inflammation by acting on keratinocytes, dendritic cells and indirectly on T-lymphocytes (10). The expression of IL-36γ is regulated by innate (via the antimicrobial cathelicidin LL37) but also by adaptive immune mechanisms (via IL-17, produced by T cells). It is therefore very likely that this cytokine most probably plays a central role in the inflammatory vicious circle of psoriasis (11).
In this cohort, IL-36γ is significantly more strongly expressed in the epidermis of patients with psoriasis-based erythroderma than in other inflammatory skin diseases, which cause the same clinical appearance. IL-36γ is expressed in 4 or more cell layers of the epidermis in half of the psoriatic cases. This pattern is not seen in any other form of erythroderma. Our data indicate that IL-36γ immunohistochemical staining could be a valuable tool to specifically identify approximately 50% of psoriasis cases among erythroderma patients and could thus help provide patients with an immediate disease-targeted therapy.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2265
REFERENCES


