


1Department of Dermatology, Institute of Clinical Research in Malmö, Skåne University Hospital, Lund University, Malmö, 2Department of Dermatology, Division of Clinical and Experimental Medicine, Linköping University, Linköping, 3Department of Dermatology, Ängelholm Hospital, Ängelholm, 4Unit of Occupational and Environmental Dermatology, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, and 5Department of Public Health and Clinical Medicine, Dermatology and Venereology, Umeå University, Umeå, Sweden
There is good agreement between dermatological staff and patients using the Hand Eczema Extent Score (HEES). The aim of this study was to assess inter- and intra-observer reliability of the HEES in dermatologists and intra-observer reliability of the HEES in patients with hand eczema. Six dermatologists assessed 18 patients twice. Only the hands of the patients were visible to the assessors. Patients performed a self-assessment twice. Inter- and intra-observer reliability was tested with intraclass correlation coefficient (ICC). The mean HEES score for all dermatologists’ assessments was 21.0 (range 3.6–46.3). The corresponding mean scores for all patients’ own assessments were 24.9 (range 4.0–54.0). Inter-observer reliability in the dermatologists’ observations ICC classification was very good, median value 0.82 (range 0.56–0.92). The overall intra-observer reliability for the 6 dermatologists’ ICC classification was very good (range 0.88–0.94). Intra-observer reliability in the patients’ 2 self-assessments ICC classification was very good (ICC 0.95). In conclusion, HEES is a reliable tool for both dermatologists and patients to grade the extent of hand eczema.
Key words: dermatitis; inter-observer reliability; intra-observer reliability; self-assessment; severity.
Accepted Aug 22, 2016; Epub ahead of print Aug 26, 2016
Acta Derm Venereol 2017; 97: XX–XX.
Corr: Annica Carlsson, Department of Dermatology, Ängelholm Hospital, SE-262 81 Ängelholm, Sweden. E-mail: annica.m.carlsson@skane.se
Hand eczema is a common (1) and frequently debilitating disease with proven impact on ability to work (2) and quality of life (3, 4). The 1-year period prevalence of hand eczema is approximately 10% in working age people in Northern Europe, with females being affected more frequently than males (1). The aetiology of hand eczema is often multifactorial and the clinical presentation varies (5). Hand eczema has a chronic, variable, relapsing course in most patients (6).
Various tools have been suggested for grading hand eczema (7–14). Most of the methods evaluate both extent and clinical signs. In a study of the long-term prognosis of hand eczema, the extent of hand eczema at baseline was shown to be a strong predictor of persistence of hand eczema after 15 years (15, 16). The same research project showed that recording morphology did not add significant information when assessing the long-term prognosis of hand eczema (16). The Hand Eczema Extent Score (HEES) (Appendix S1), a simple method of scoring the extent of hand eczema (11, 12), has been shown to give good agreement between dermatologists and nurses as well as between dermatologists and patients. It is important to evaluate the inter- and intra-reliability of HEES in a group of dermatologists. This should be performed in accordance with the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) (17). For follow-up of the course of the disease, it would be valuable if the patients could make self-evaluation of their hand eczema.
The aims of this study were to assess inter- and intra-observer reliability of the HEES in dermatologists and the intra-observer reliability of the HEES in patients with chronic hand eczema.
Patients with bilateral hand eczema from 2 dermatology clinics in Sweden (Malmö and Ängelholm) were informed about and invited to participate in the study, which was approved by the Regional Ethical Review Board in Lund (1-2012). A telephone call to the patient one week before the study took place confirmed that both hands still were affected. A further inclusion criterion was sufficient command of Swedish to ensure comprehension of oral and written information/instructions. Written consent was obtained from all participating patients.
The study was conducted at the dermatology clinic, Skåne University Hospital, Malmö, on 2 occasions (April and November 2012) with 11 and 7 patients, respectively. On the first occasion it was not possible assemble the total number of patients needed according to the power calculation. A second occasion was therefore planned for the autumn, since hand eczema often tends to be better in summertime. Six experienced dermatologists performed HEES twice in each patient; before and after lunch. A nurse (AC) informed all the patients, orally and in writing, about study procedures before the first scoring session. The patient’s placement by nurses in rooms (1 or 2 patients per room) was dictated by the order in which they arrived in the clinic. Each patient also took a lottery ticket, which randomized them for placement on the second assessment. The patients sat behind a screen with only their hands visible for the observers sitting in front of the screen (Fig. S1). The patients were asked not to wear any recognizable items, such as rings, bracelets or nail polish, on their hands. Tattoos were an exclusion criteria. The dermatologists were instructed to avoid communication with the patients, other than asking them to show or to turn their hands. The HEES form was completed and sealed in an envelope by the observers at the completion of the assessment and by the patients at the time of the self-scoring at the beginning of each scoring session. When all 6 dermatologists had completed the assessments in one room, they moved at the same time to the next room. Dermatologists and patients did not meet each other until the second scoring session was finished. The interval between the 2 assessments per patient performed by dermatologists was between 90 and 240 min. The dermatologists were not permitted to discuss the assessments during the day.
HEES, based on the notation of any sign of eczema at anatomical sites on the hands, was used (11, 12, 16). The scoring system was initially developed by Meding & Swanbeck (18). A facilitated layout was later developed for self-assessment by patients (11, 12) (Appendix S1). The scoring system was based on one possible point for each anatomical site involved, with the exception that the score for the back of the hand and the palm generated 0 (absent), 2 (for less than two-thirds involvement) or 4 (for more than two-thirds involvement) points for each anatomical site. The range of possible score for each hand is 0–37, with a maximum of 74 for both hands. In previous publications the extent of involvement is grouped in 4 categories: very mild (1–3), mild (4–5), moderate (6–12) and severe (> 13) (18).
The sample size calculation is based on the assumption that the ICC between and within observers would be at least 0.8. To achieve an estimate of the ICC with a precision of ± 10% (95% confidence interval (CI) 0.81–0.99) 32 observations are required. As each hand was counted as one observation, 16 patients with eczema on both hands were needed. To allow for drop-outs it was planned to include 20 patients.
Inter- and intra-observer reliability were assessed using ICC (19). The calculation is based on a 2-way mixed model and absolute agreement. ICC measures the degree of agreement between different observers when they examine the same patient and the consistency of each observer’s repeated assessment of the same patient. ICC assumes that the scale is continuous. HEES is an ordinal scale variable, but since the underlying scale, the area of a hand affected by hand eczema, is continuous, we believe that HEES is a good approximation of the underlying scale and ICC is chosen as the agreement measure.
A Bland-Altman (B-A) plot is a common way to illustrate agreement between raters and displays the difference between 2 raters scoring vs. the mean of the raters scoring (20).
B-A plots for the “best” and “worst” ICC outcomes are shown. In the B-A plot the limits of agreement (LoA) are also shown. Between those limits we can expect approximately 95% of the differences between the scoring of 2 raters.
ICC values are interpreted as follows: ≤ 0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good, and 0.81–1.0, very good (21). All statistical analyses were performed with SPSS version 22.0.
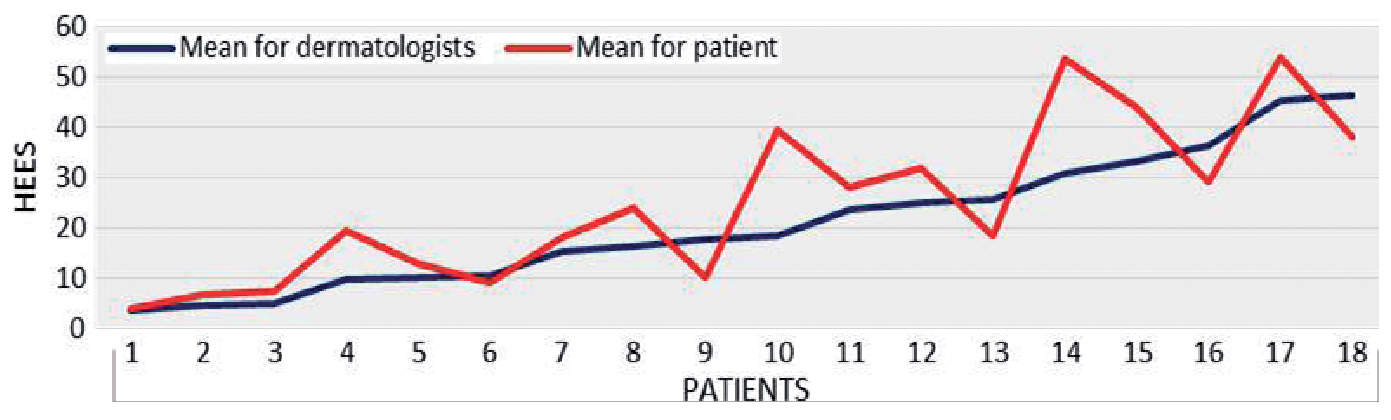
Eighteen patients (14 females, 4 males) with a mean age 49 years (range 28–72 years) participated in the study. The results shown for the HEES are for 18 patients measured twice, i.e. 36 observations; however, the ICC is calculated on scores from each individual hand, i.e. 72 observations. The mean value of the HEES for all dermatologists’ assessments was 21.0 (range 3.6–46.3). The corresponding mean scores for all patients’ own assessments was 24.9 (range 4.0–54.0). The distribution of the extent of eczema in our study includes the categories very mild, mild, moderate and severe. Fig. 1 shows the mean value for each patient judged by the dermatologists compared with the mean value assessed by the patients themselves. The mean values of HEES in the 2 assessments, performed by dermatologists and by patients, are shown in Table I. The Table also shows the variability in scoring between dermatologists. There was a wide spread of extent/severity of hand eczema in the patients on both of the 2 study occasions.
Fig. 1. Mean value of Hand Eczema Extent Score (HEES) (both hands), assessed by dermatologists, for all patients (n = 18) in ascending order, compared with mean values assessed by the patients themselves.
Table I. Hand Eczema Extent Score (HEES) for the 6 dermatologists (D) and the 18 patients. Intraclass correlation coefficient (ICC), (test–retest) calculated for each dermatologist and for the patients’ 2 assessments
ICC between dermatologists for assessment pairs (15 pairs, D1–D2, D1–D3, etc.) varied from 0.56 (95% CI 0.21–0.75) to 0.92 (95% CI 0.88–0.95) (Table II). The differences in scores between the 2 dermatologists (D5 vs. D6) with the lowest ICC is shown in Fig. 2A. Fig. 2B shows the differences in scores between the 2 dermatologists (D2 vs. D4) with the highest ICC. The overall inter-observer reliability ICC classification was very good, the median value of ICC was 0.82 (95% CI 0.54–0.92).
Table II. Intraclass correlation coefficient (ICC) and 95% confidence interval (CI) for the pairs of dermatologists (D)
Fig. 2. Differences in scores between the 2 dermatologists with: (A) lowest intraclass correlation coefficient (ICC) (0.56); and (B) highest ICC (0.92).
The ICC between the 2 assessments by each dermatologist is shown in Table I. The overall intra-observer reliability for the 6 dermatologists’ ICC classification was very good (range 0.88–0.94).
Intra-observer reliability for the patients’ 2 self-assessments (Table I) ICC classification was very good, the ICC was 0.95 (95% CI 0.90–0.97).
In this study the reliability of the HEES was tested for the first time. The intra-observer reliability in dermatologists’ and patients’ ICC classifications was very good. In dermatologists the inter-observer reliability in ICC classification was very good when median values of ICC are considered. However, some individual values were lower than 0.7 and our overall estimation is that the inter-observer reliability should be classified as good. Thus HEES is proven to be a reliable tool for assessing extent of hand eczema. In a previous study of HEES we found a good agreement between dermatologists and patients as well as between dermatologists and nurses (11, 12).
The study design with blinded assessors guaranteed unbiased and independent scoring of the extent of hand eczema. The interval between the 2 assessments was chosen for practical reasons. Factors of importance were that the eczema extent should be the same and there should be enough time to relocate and change the order of the patients.
The generalizability of our results could be questioned since there were only 6 dermatologists participating, which might reduce inter-observer variability. If HEES is used exclusively in patients with a great extent of hand eczema, the variability in extent scoring might be smaller than was observed in this study, where the range of HEES included all the categories; very mild, mild, moderate and severe (18). Previously shown agreement between dermatologists and nurses as well as dermatologists and patients without special training in using the instrument, indicates that HEES could be widely used (11, 12). In the present study dermatologists as well as patients also used HEES without encountering any problems.
Scores for quantifying hand eczema have been used predominantly to evaluate the outcome of treatment. Many tools for quantifying hand eczema are used, but there is no consensus as to which method is to be preferred (22). The Hand Eczema Severity Index (HECSI) (7), a widely used tool for estimating severity of hand eczema, includes registration of extent, morphology and intensity. Osnabrück Hand Eczema Severity Index (OHSI) (23) and Hand Eczema score for occupational screenings (HEROS) (22, 24) also value extent, mor-phology and intensity as well as Manuscore (25), which also includes the subjective symptom itching. HECSI has been shown to have a higher correlation with Investigator Global Assessment (IGA) than Hand Eczema Area and Severity score (HEAS) and a 3-item score, which is a reduced HECSI (26).
When rating severity of hand eczema it is important to consider objective as well as subjective parameters (27). HEES is a tool constructed for assessment of the extent of hand eczema and is an objective way to grade the eczema. The patient’s experience of the disease is usually expressed as health-related quality of life (HRQoL). Dermatology Life Quality Index (DLQI) (28) is the most well-known tool for assessment of QoL in dermatology. A positive correlation between HEES and DLQI (0.31) has been observed in a study on hand eczema patients (29). There was, however, no significant correlation between HECSI score and DLQI in another hand eczema study (30). Recently a disease-specific HRQoL instrument for hand-eczema was published, which covers the domains of symptoms, emotions, functioning and treatment and prevention (31). This instrument is more specific to measure QoL for patients with hand eczema, but is not yet used together with HEES.
Assessment of inter-observer agreement on clinical signs has been found to be lower than agreement of extent and anatomical location (7). The difficulty in identifying clinical signs was emphasized previously in a study showing poor agreement between patients’ reports and doctors’ observations of clinical signs of hand eczema (32). HEES is a measurement of the extent of hand eczema and does not involve clinical signs. This makes HEES easier to use in patient self-assessment. Until now the sensitivity to change has not been studied, but evaluation of this aspect would be valuable in a clinical context. In the clinical setting morphological aspects not covered by HEES can be important, but the magnitude of this problem needs further evaluation.
Five methods have been tested previously for reliability, the Manuscore (25), HECSI (7), photographic guide (8), OHSI (23) and HEROS (22, 24). Inter-observer reliability has been analysed in 4 studies (7, 8, 23, 25) including patients with different severity of eczema and in one study (24) including workers with mild eczema. Inter-observer reliability was good to very good in all these studies. Intra-observer reliability was analysed in 3 studies (7, 8, 24); 2 studies (7, 8) include patients with different severity of eczema, and one (24) includes workers with mild eczema. Intra-observer reliability was very good in these 3 studies. Studies including the same category of patients are required when comparing different tools for quantifying hand eczema.
In summary, HEES is a reliable tool for grading the extent of hand eczema. This scoring system reliably avoids observer bias and takes only a short time for assessment. HEES can conveniently be used by dermatologists or by patients themselves to follow the course of chronic hand eczema or the results of interventions.
The authors would like to thank the patients for participating in this study. The authors acknowledge Ann-Kristin Björk, Margareta Lundahl, Ulla-Maj Persson and Lila Baraslievska who helped with food and beverages. The study was supported by grants from the Edward Welander and Finsen Foundations and the Research and Development Fund of Ängelholm Hospital.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize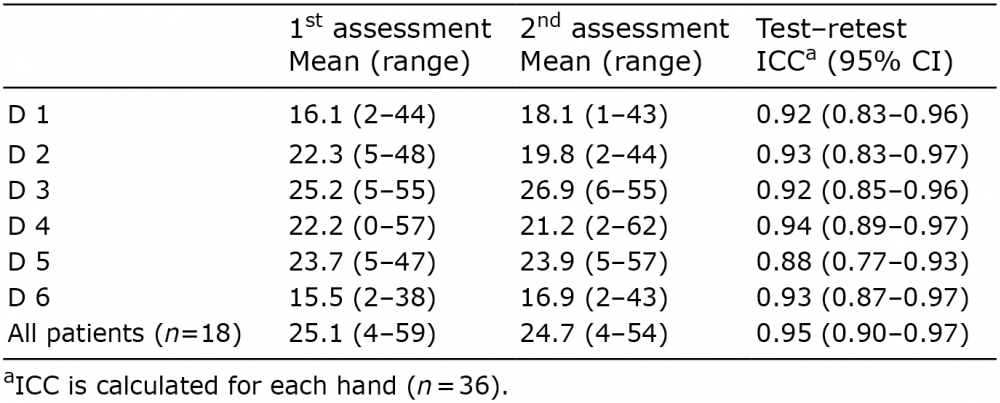 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize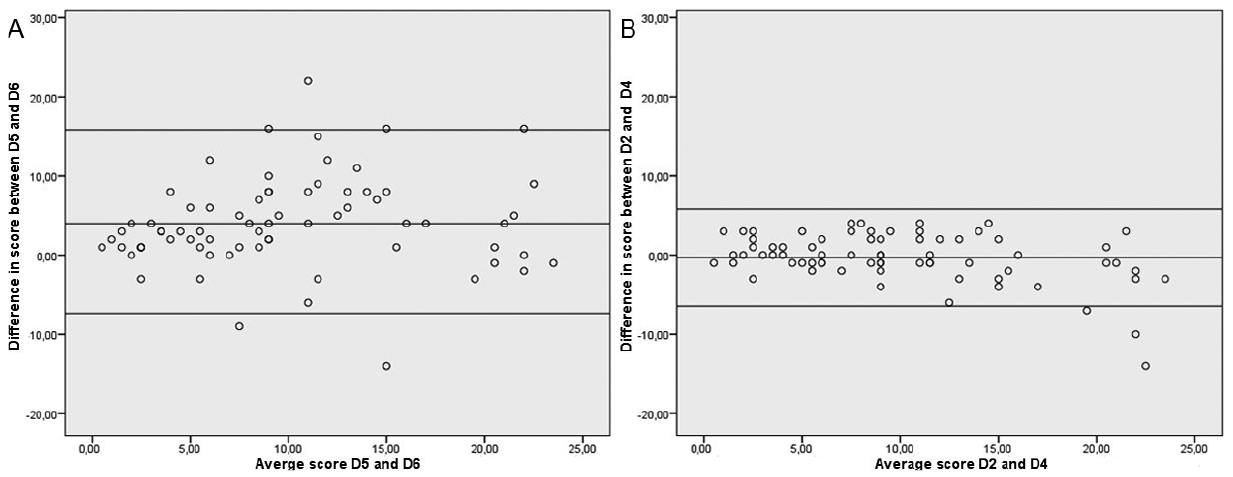 Click to show fullsize
Click to show fullsize