


1Research Unit, Fundación Academia Española de Dermatología y Venereología, Ferraz 100, 1º izda. Madrid, Spain, 2Dermatology and Venereology Department, Umeå University Hospital, Umeå, Sweden, 3Department of Dermatology, Complexo Hospitalario Universitario de Vigo (CHUVI), Vigo, Spain, 4Centro Studi GISED, Fondazione per la Ricerca, Ospedale Maggiore, Bergamo, Italy, 5German Center for Health Services Research in Dermatology, University Clinics of Hamburg, Hamburg, Germany, 6Department of Dermatology, Hospital Universitario La Princesa, Madrid, Spain, Departments of Dermatology, 7Roskilde Hospital, Roskilde, Denmark, 8Skin and Cancer Foundation, St Vincent’s Hospital Melbourne, University of Melbourne, Australia, 9Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands and 10Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, USA, and 11Department of Quality Measures and Research, Clalit Health Services. Tel Aviv, Siaal Research Center for Family Medicine and Primary Care, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel. E-mail: pauladavilaseijo@gmail.com
Accepted Nov 23, 2016; Epub ahead of print Nov 24, 2016
PSONET is an international network of independent partners that aims to document “real-life” use of systemic drugs for psoriasis in different countries (1–3). Differences in how the registries’ populations are treated have implications for the analysis of data (as these factors could act as confounders for risk estimates), for the generalizability of results from individual registries, and for understanding dermatologist behaviour in different healthcare systems and countries.
The objective of this study is to describe and compare the characteristics of patients treated with classic and biological agents for psoriasis in participating registries.
The study population are patients with moderate-to-severe psoriasis, over 18 years of age, who have received systemic treatment for psoriasis. Except for Clalit Health Services, which utilizes administrative data, participating registries are cohort studies that enrol patients when they first receive, or are currently receiving, a study drug.
Baseline data from 7 countries’ registries included the Netherlands (Academic Medical Centre (AMC) psoriasis registry) (4, 5), Australia (Australasian Psoriasis Registry), Spain (BIOBADADERM) (6, 7), Israel (The Clalit Health Services), Denmark (DERMBIO) (8, 9), Germany (PSOBEST) (10) and Italy (PSOCARE) (11, 12).
Participating registries provided aggregated summary data concerning baseline, demographic and disease characteristics of their cohort. Table SI gives information about the organization of each registry. Inclusion criteria for the different registers are earlier described in (3). In general, they include all biological treatments consecutively and a convenience sampling of classic drugs. All registries received approval from their local ethics committee, and comply with the principles of the Declaration of Helsinki.
Pooled analyses were performed using Stata 12.1 software (StataCorp College Station, TX, USA). To measure the association between exposure to biologics or classic systemic therapies and a priori defined variables, differences in means between groups were used for continuous variables, and odds ratios (OR) for categorical variables. To pool data from registries, forest plots were used and a random-effects meta-analysis was conducted to describe differences among groups exposed to biologics or conventional therapies. Pooled estimates of effects were produced if results were not too heterogeneous (I2 < 60%). Some registries were not able to provide data on all of the defined variables. Due to the lack of enrolment of patients receiving classic systemic therapy, AMC psoriasis registry data were not included in the forest plots and in comparisons of exposure cohorts. In all the other registries, if a patient began in the non-biological therapy group and subsequently received a biologic drug, his or her characteristics contributed to both groups in the analysis.
From the start of each registry to August 2012, a total of 20,232 patients had been enrolled in the registries and provided baseline information. This included 9,668 (47.8%) initially treated with biologics and 10,564 (52.2%) starting classic systemic therapies.
Demographic and disease characteristics are summarized in Tables SII and SIII.
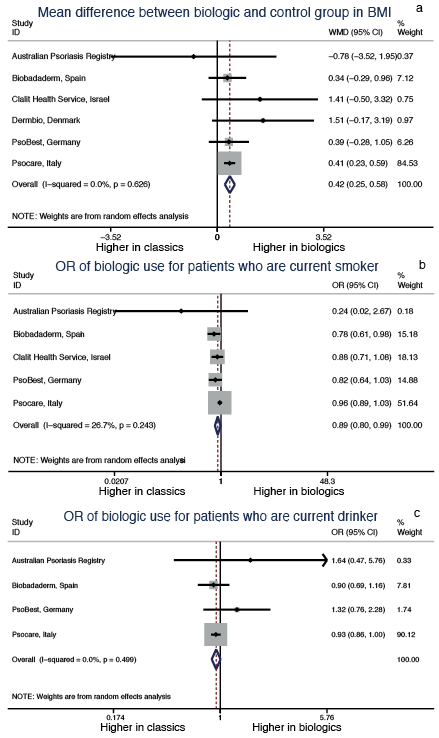
Some differences between patients receiving biologics and those receiving classic drugs were homogeneous between registries (I2 ≤ 60%). These are presented in forest plots in Fig. 1, which includes I2 values, and pooled estimates. Overall, patients on biologics were 0.42 units of body mass index (BMI) heavier than those on classic systemic drugs (95% CI: 0.25–0.58). The OR of males vs. females receiving biologics was 1.08 (95% CI: 0.94–1.24). Use of biologics was slightly less likely in current smokers (OR 0.89, 95% CI: 0.80–0.99).
Fig. 1. Forest plot showing the overall result in psoriasis characteristics of patients without substantial heterogeneity (I2<60%) in both biologic and control group among different registries: (a) differences in body mass index (BMI) between biologic and conventional treatment groups. (b) Odds ratio (OR) of biologic use compared with conventional treatment among current smokers. (c) OR of biologic use compared with conventional treatment among current
drinkers.
Fig. S1 shows the results in each registry, but not pooled estimates, because heterogeneity was too high (I2 > 60%). Age at entry, age at diagnosis and Psoriasis Area and Severity Index (PASI) at entry were too heterogeneous among registries to be combined in the meta-analysis. Italian and Spanish patients on biologics had a PASI significantly higher at entry and were significantly younger at diagnosis than those receiving classic systemic therapies. Few registries reported measurements of body surface area (BSA) and Dermatology Life Quality Index (DLQI) or SKINDEX, making comparisons between registries difficult.
Patients with psoriatic arthritis or nail disease were more likely to receive biologics than classic therapies in almost all registries, but the results were heterogeneous despite the significant OR favouring the usage of biologics in most of them. In registries from Italy and Spain, patients with psoriasis different from plaque psoriasis were significantly more likely to receive conventional drugs.
In agreement with the findings of a previous PSONET analysis (1), the current study revealed that wide between-country heterogeneity exists in the distribution of covariates potentially influencing treatment selection (e.g. age, PASI and proportion with non-chronic plaque psoriasis). Beyond between registry variability, the current study found that some covariates are related per se with the odds of receiving a biologic or a classic treatment in most registries, e.g. BMI, psoriatic arthritis, nail disease or proportion of current smokers.
The strengths of this study are the increased power obtained from multiple registries compared with using each separately, the ability to describe and quantify between-country differences, and the use of a meta-analytical approach, in which each registry acts as its own control, which limits the risk of biases related to differences between registries. In addition, meta-analysis is a good way to define and quantify heterogeneity and to balance out differences in sizes among the registries.
Study limitations are: missing data from some registries, missing data on some predefined variables and that only univariate analysis was performed and we could not rule out that the factors we found as being associated with treatment choices were, in fact, intercorrelated and not independently associated with the treatment selection. A further limitation is that we could only analyse commonly measured and coded variables. Finally, the data were not updated. This delay is due to the extreme difficulty in combining data from different national registries. But because of the already high number of participants, we consider that this should not affect the results and overall conclusions.
Methodological differences might explain some of the differences found. This is probably the case for the heterogeneity of the percentage of patients with psoriatic arthritis or in PASI values. PASI values are also influenced by the lack of wash-out periods before starting a new therapy (leading to variability and PASI decrease) in real-world registries and by the fact that a minimum PASI is mandatory to prescribe biologics in some countries (possibly leading to a factitious increase). Single outlying results may also hide otherwise homogenous effects, e.g. only in the Danish registry is there no greatly increased use of biologics for psoriasis arthritis; thus, the otherwise highly significant prediction by psoriasis arthritis disappears.
Knowledge of the factors related to drug selection is important in order to plan statistical analysis of observational data (13). Each registry could use this information to develop strategies for dealing with prescription bias, using methods such as propensity scores (14). Identification of differences in the international usage of drugs can be useful for interpretation of observational studies (e.g. generalization of results) (15), adds knowledge and understanding of different healthcare systems and might indicate areas for improvement in patient management.


 Click to show fullsize
Click to show fullsize