


1St. John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Foundation Trust, London, UK, 2Unit for Population-Based Dermatology Research, Department of Paediatric Dermatology, St John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, 3Department of Non-communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK, 4Catedra de Analisis Estadistico y Big Data, Catholic University of Murcia, Spain, and 5Department of Dermatology, Institute of Clinical Research in Malmö, Lund University, Skåne University Hospital, Malmö, Sweden
To date the efficacy and safety of topical timolol in the treatment of infantile hemangioma has not been reviewed and analysed systematically. We collated all published data on the efficacy and safety of topical timolol in the treatment of infantile hemangioma. A total of 31 studies with 691 patients were included. The fixed effects pooled estimate of the response rate defined as any improvement from baseline of infantile hemangioma after treatment with topical timolol was significant (RR = 8.96; 95% CI 5.07–15.47; heterogeneity test p = 0.99), and the treatment was overall well tolerated. However, the quality of evidence was low to moderate. Topical timolol is an effective treatment for small infantile hemangioma, with no significant adverse effects noted. However, there is still a need for adequately powered randomised controlled trials.
Key words: infantile hemangioma; timolol; beta-blocker.
Accepted Apr 18, 2017; Epub ahead of print Apr 19, 2017
Acta Derm Venereol
Corr: Dr Carsten Flohr, Director, Population-Based Dermatology Research Unit, St John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Foundation Trust, Westminster Bridge Road, London SE1 7EH, UK. E-mail: carsten.flohr@kcl.ac.uk
Infantile hemangiomas (IHs) are benign proliferation of endothelial cells arising in the first 8 weeks of life as an area of telangiectasia or discoloration (1). IH are the most common benign tumours of infancy (2). Their life cycle is characterised by an early proliferative phase (6–12 months) followed by gradual involution, leading to complete regression in most cases (5–9 years) (1).
The incidence of IH in one-year-old children is estimated to be 5 to 10% (3). Preterm infants with a birthweight of < 1,000 g have even a higher risk of 23% (4). There is female preponderance and predilection for Caucasians (5). Positive family history in first degree relatives and periconceptual use of drugs increases the risk of IH (6). Although most hemangioma occur sporadically, autosomal dominant transmission has been reported (7). Old maternal age, placenta previa, and pre-eclampsia have been associated with IHs (8).There is an increased risk following amniocentesis and even a greater risk after chorionic villus sampling (CVS) (9). Embolization of angioblasts or endothelial cells from placenta to fetal skin during CVS might lead to multiple hemangiomas on the head, neck and thorax (10).
While the majority of IHs regress spontaneously, approximately 10% require intervention (11). Typical indications for oral beta-blocker therapy include functional impairment (e.g. periocular IH causing amblyopia, nasal IH causing nose deformity, lip IH leading to feeding difficulties, and auricular IH causing deafness), and IH in life threatening anatomical locations (lung IH causing respiratory distress, obstructive subglottic IH, large cutaneous IH causing hepatic dysfunction and cardiac insufficiency) (11, 12). However, oral beta-blockers can have potential side-effects, such as a reduction in blood pressure and heart rate, even if the risk is small (13). Therefore, the topical application of a beta-blocker has been suggested as a suitable alternative, in particular for superficial IH (14). In 2010, Guo & Ni (15) presented the first report of successful topical timolol treatment in a resolving IH. Since then, several case reports and case series have claimed efficacy of topical timolol, making this a potential first-line agent for the treatment of superficial IH (13).
While there are American and European consensus guidelines for the use of oral beta-blockers (13, 16), there is still very little guidance on the optimal use of topical beta-blockers. To inform clinical practice and guidelines development, we therefore conducted a systematic review and meta-analysis of the literature on the efficacy and adverse effects of topical timolol for the treatment of IH.
This review was registered with the University of York Centre for Reviews and Dissemination (registration No. CRD42015019225), and we followed the PRISMA guidelines on the conduct of systematic reviews throughout. The Cochrane Library, OVID Medline (1946–May 2015) and OVID Embase (1980–May 2015) databases were systematically searched for original publications using the following syntax: (hemangioma OR hemangiomas OR haemangioma OR haemangiomas) AND (timolol OR beta-blocker OR beta blockers). All randomized controlled trials (RCTs), case-control studies, case series and case reports documenting the treatment response of IH to any preparation of topical timolol as mono-therapy were eligible for inclusion. There was no restriction with regard to publication period, population size, or Fitzpatrick skin type. Our outcomes were treatment efficacy of topical timolol in the resolution of IH (primary outcome) and adverse events of timolol as well as rebound growth after discontinuation of treat-ment (secondary outcomes). Papers that did not document the clinical response to timolol and that were not available in English translation were excluded.
The Cochrane Risk of Bias Assessment Tool for Non-Randomized Studies of intervention (ACROBAT-NRSI) was used to assess study quality (17), together with GRADEpro to create a summary of findings table (SoF). The quality of evidence for each predefined outcome was rated as ‘high’, ‘moderate’, ‘low’ or ‘very low’(18).
Response rates and their corresponding 95% confidence intervals (CI) were initially calculated for individual studies. Then fixed and random effects model were used to pool response rates across studies. The degree of heterogeneity across the trials was calculated using the I-squared ( I2) statistic and the p-value from the Q-statistic. Seven studies did either not have a control group (case series) or had a control arm with an additional treatment. To include those studies without a control group in the final meta-analysis, we imputed a control group to each study by using the mean rate of improvement observed in the control arms of the 3 best conducted studies included in the systematic review. The minimum number of individuals was used to reach this mean rate in the imputations, thus allowing for a large uncertainty.
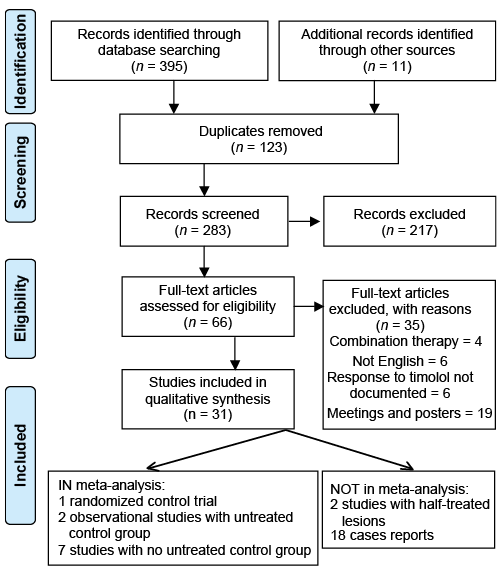
After screening titles and abstracts of 406 articles by two independent assessors (MK and AB), 66 studies were selected for reading of the full text. Of the 66 studies, 31 studies with 691 patients were included in the systematic review (15, 19–48) and 10 contained data that could be included in the meta-analysis (24, 25, 32–35, 39, 42, 46, 48; Fig. 1). A GRADE assessment could be conducted on the 6 studies with comparator/control groups (23, 24, 35, 36, 42, 48).
Fig. 1. Flow diagram of preferred reporting items for systematic review and meta-analyses for the systematic literature search.
Unless otherwise stated, the studies used timolol ophthalmic eye drops. Only one RCT compared topical timolol 0.5% BD (two times daily) with placebo (25). Two studies compared timolol with observation alone (24, 48), one study used topical timolol in conjunction with topical imiquimod (36), and one non-randomised study employed timolol together with PDL Nd:Yag laser therapy (42). Another was a case report comparing timolol and propranolol in two separate patients (26). In two studies, IH was arbitrarily divided into two halves (49, 50). Timolol was applied to one-half and imiquimod to the other, or the other half acted as control site. These papers were excluded because there was no accurate way to prevent cross-contamination, and this is likely to have influenced the study outcome. Patient age when timolol was started ranged from 17 days to 13 months (mean age 4.02 months), with a majority being females (67.9%). Most were superficial IH (87.8%), except two case reports in which only deep IH were treated (41, 47). Most of the studies were done in Europe (12 studies) followed by the USA (8 studies) and Asia (6 studies), but participant ethnicity and Fitzpatrick skin type were often not specified. In 25 studies (80.6%) with 421 cases, timolol 0.5% was used. The 0.1% preparation was used in 5 studies with a total of 40 cases (23, 29, 39, 40, 44), whereas topical timolol 0.25% was used in only one study with 13 cases (24). Twenty-five studies with 170 cases used topical timolol BD and two studies applied topical timolol TDS (3 times daily) (152 cases) (37, 48). Timolol gel forming solution was used in 6 studies with 92 cases (23, 31, 32, 41, 44, 45). Moehrle et al. (32) manufactured a special timolol containing gel with timolol 0.5% eye drops 10.0 g and methyl hydroxypropyl cellulose 0.4 g. The treatment dose was titrated up from 0.25 % to 0.5% in one study (26). In all studies, treatment was on an outpatient basis with a mean duration of 4.11 months (range two weeks to 12 months). Primary indications for treatment were suspected functional and cosmetic disfigurement, risk of ulceration, infection, amblyopia and concern about adverse effects with other treatments.
Resolution of IH. All studies used different methods of assessing the effectiveness of treatment. The hemangioma activity score (HAS) was utilized by two studies (34, 37). The result of the 3 studies using a visual analogue scale (VAS) is shown in Fig. 2 (23, 36, 37). In the remaining studies, the clinicians visually assessed improvement and documented it as percentage improvement, with the aid of clinical photographs (Table SI and Table SII).
Fig. 2. Mean of visual analogue scale (VAS) percentage change from baseline of the 3 studies that used this outcome. The numbers in bold represent the mean VAS percentage of each study. Chakkittankandiyil et al. (23) reported that timolol 0.5% had more effect than timolol 0.1%. Qiu et al. (37) reported timolol 0.5% to be more effective than topical imiquimod.
The clinical trial and two observational studies with untreated control groups had all relative risks (RR) > 1 with overlapping CI (Fig. S1). A test for heterogeneity showed no statistical evidence of differences between these RR (p = 0.71, I2 = 0%), therefore we estimated the mean of these risk ratios with the technique known as “fixed effect model meta-analysis” obtaining an RR of 9.04 (95% CI 3.22–25.41). We also estimated the mean rate of improvement only in untreated patients across these 3 studies (Fig. S2). This mean improvement was 0.09 (9%) with no evidence of heterogeneity between studies (p = 0.71, I2 = 0%). We then imputed a control group in each of the other 7 studies that did not have it originally by including 11 untreated patients, one of which showed improvement. This assumes the same improvement rate than the mean in the observed studies (1/11 = 0.09) with the minimum possible sample size.
Finally, a meta-analysis of the RR between the two arms in all 10 studies with the imputed data produced a mean RR of 8.86 (95% CI 5.07–15.47) (Fig. 3), which is very similar to the RCT and the two non-randomised controlled studies. This analysis showed no evidence of heterogeneity (p = 0.99, I2 = 0%), and the random effects model produced very similar results.
Fig. 3. Meta-analysis of all 10 studies, including imputed data from studies without control group. The meta-analysis of the relative risks (RR) between the two arms in all 10 studies with the imputed data produced a fixed effects estimate of 8.86 (95% confidence interval (CI), 5.07–15.47). This analysis showed no evidence of heterogeneity (p = 0.99, I2 = 0%).
Sleep disturbance was the only systemic adverse effect reported in two cases (23, 42). Rebound growth occurred in 4 patients from 3 studies (27, 32, 46). In 3 patients treatment was restarted, still leading to complete resolution of the IH (32, 46). The mean period of follow-up after discontinuation of treatment ranged from 3 to 6 months in the studies that did report them. The majority of the studies reported no long-term follow-up. There were only 8 cases of deep IH, with complete resolution in 7 cases (23, 24, 41, 47). Unfortunately, the overall case numbers are too small to draw any firm conclusions with regard to potential differences in treatment response in relation to IH depth or size, age when treatment was started and treatment length and how this impacted on treatment response and rebound in the few cases where this was observed.
Risk of bias and GRADE assessment. The risk of bias could only be formally assessed in the 6 studies with control/comparator groups (Table SIII) (23, 24, 35, 37, 42, 48). The overall risk of bias was serious mainly due to confounding, selection of participants and lack of a per-protocol analysis. The GRADE outcome parameters were categorized as critical (treatment effect and adverse effects), important (resolution > 50% from baseline and complete resolution) and less important (rebound growth and parents’ assessed improvement with topical timolol) and are summarized in Table SIV. The overall quality of evidence was moderate to low quality.
To the best of our knowledge, this is the first systematic review and meta-analysis focusing on topical timolol for the treatment of IH, summarising data from 31 studies with 691 patients. Topical timolol 0.5% is a promising and effective treatment modality, with a 91% resolution rate in pooled meta-analysis. The expected efficacy of control arms was estimated to be 9%, i.e., we would expect to see a mean of 9% clearance of IH in patients who received placebo or no treatment during the study. The degree of resolution was significantly greater in the treatment than in the non-treatment group. This further verifies the efficacy of topical timolol over placebo/observation.
We followed the PRISMA guidelines for systematic reviews. Study selection was performed independently by two authors, following a priory agreed data extraction protocol, which was published on the PROSPERO website. The online search was supplemented by an extensive hand search of the literature. A key but unavoidable difficulty was the heterogeneity of the included studies with regard to dosing, duration of treatment, study endpoints and monitoring frequency. As a result, we had to combine the only RCT with observational study evidence. For the case series that did not have a control group we imputed the control group effect from controlled studies.
Lack of comparator groups limited formal GRADE assessment to only 6 studies. The quality of evidence was low to moderate quality. Bias in selection of participants, lack of per-protocol analysis and confounding increased overall risk. However, the homogeneity of individual study results, in keeping with the only RCT (25), underlines the validity of our findings.
Main weaknesses across all studies were the low number of participants and lack of long-term follow-up. Sleeping disturbance was the only reported side effect in 2/475 cases. Whether the sleeping disturbance was specifically due to topical timolol cannot be said with certainty, given how common this is in otherwise healthy infants, but the favourable side effect profile suggests that no specific side effect monitoring is required, different from oral beta-blocker therapy.
No side-effects were noted when topical timolol was applied on mucosal surfaces, like the lips or on ulcerated areas. It is established that the greater viscosity of gel-forming solution potentially decreases the systemic absorption and leads to lower peak plasma concentration (0.28 ng/ml), but more information about the pharmacokinetics of topical timolol on hemangiomas is needed (51).
Most studies used topical timolol 0.5% BD, and the medication is well-tolerated at this dose. The IH was completely resolved in 5 studies (40 cases) that used 0.1% preparation (23, 29, 39, 40, 44). In the only study that used 0.25% topical timolol 12/13 cases responded (24). This information is not enough to make comparative assessment between different doses of topical timolol. In two studies, deep IH were exclusively considered and good response was documented in all 5 cases treated with topical timolol 0.5% BD (41, 47). But 5 is a small number of cases to extrapolate results from and more studies are required in this subgroup analysis.
Although both the American and European consensus groups highlight the potential of topical timolol in treating IH, they do not provide guidelines on its use (13, 16). Our study provides validation on the efficacy and safety of topical timolol in the treatment of superficial IH. This can further support the development of future guidelines on the use of topical timolol in the treatment of IH (52).
However, there is a need for a well-designed and adequately powered placebo-controlled RCT, using clear diagnostic criteria and validated outcome measures. Such a study should also explore the optimal duration of treatment and treatment strength as well as the impact of IH size and depth on treatment response.
While the majority of IH do not require treatment as they spontaneously regress, a minority may require intervention to prevent distressing complications.
Having looked at the evidence that has emerged since the first use of topical timolol, the inferences have been favourable. This study provides validation on the efficacy of topical timolol for superficial, localised, small and uncomplicated IH. Topical timolol also appears safe and well-tolerated, as no overt clinical evidence of adverse effects was noted. However, while topical timolol appears to be effective in particular for superficial IH, we caution against using it when systemic treatment is clearly warranted due to functional impairment, anatomical location, size, or hepatic dysfunction and cardiac impairment.
This study highlights the need for a formal randomised control trail to further establish the efficacy of topical timolol over placebo/observation or other treatment modalities, and its long-term safety, monitoring, duration of treatment, dosing and appropriate indications for topical beta-blocker use. The findings in this study can also aid the formulation of treatment guidelines for IH.
CF holds a UK National Institute for Health Research (NIHR) Career Development Fellowship (CDF-2014-07-037). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the UK Department of Health.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize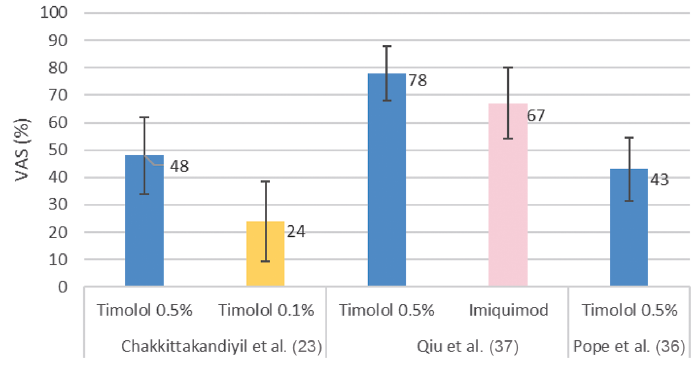 Click to show fullsize
Click to show fullsize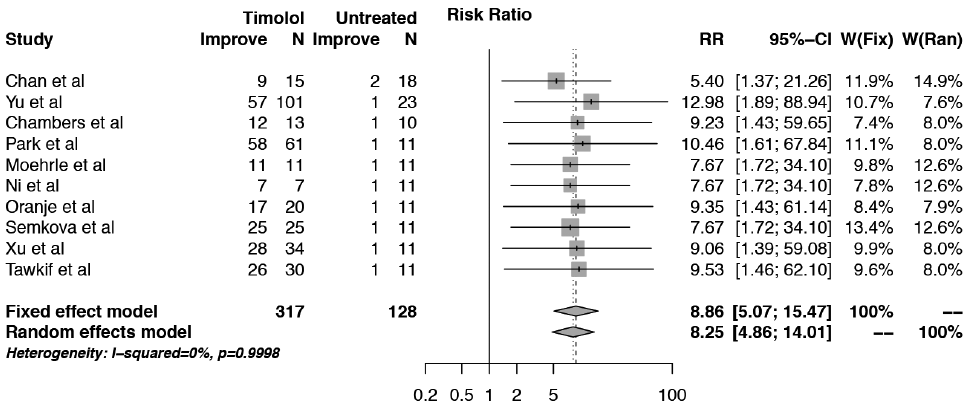 Click to show fullsize
Click to show fullsize