


Departments of 1Dermatology and 5Pathology, Maastricht University Medical Centre, P. Debyelaan 25, NL-6229 HX Maastricht, 2GROW Research Institute for Oncology and Developmental Biology, 3Department of Dermatology, Radboud Medical Centre, Nijmegen, and 4Department of Epidemiology, Maastricht University, Maastricht, The Netherlands. E-mail: maud.jansen@mumc.nl
Accepted Aug 23, 2017; Epub ahead of print Aug 23, 2017
Bowen’s disease (BD) is an intra-epidermally located squamous cell carcinoma (SCC) in situ, which occurs mostly on sun-exposed areas (1–4). Several treatment modalities are described, including surgical excision (SE), imiquimod, 5-fluorouracil (5-FU), photodynamic therapy (PDT), curettage, and cryotherapy (4–8). The major advantage of SE is histological evaluation. However, SE comes with complications and scarring. Topical therapies are less invasive, often have cosmetic superiority, enable treatment of multiple tumours at once and might be preferable for tumours in locations where excision may be complicated by delayed wound healing.
The clinical efficacy of 5-FU and PDT, compared with SE, was analysed in a large study population at our department.
Patients were retrospectively selected from the histological database from the Pathology Department of the Maastricht University Medical Centre (MUMC+), Maastricht, The Netherlands. Patients eligible for inclusion were those diagnosed with a histologically confirmed BD between 1 January 2008 and 31 December 2013 and treated by dermatologists. Exclusion criteria were: patients with BD on genitalia/mucous membranes or lesions found nearby an invasive skin cancer. Patient, tumour, and treatment characteristics were reviewed from medical records. The study was approved by the local Medical Ethics Committee.
Tumours were excised with a 5-mm safety margin, followed by routine histological examination. For PDT, application of aminolaevulinic acid (ALA) or methylaminolevulinate (MAL) cream was followed by illumination (Aktilite®, 630 nm; Galderma, SA, Lausanne, Switzerland) and repeated after one week (4, 9). For 5-FU, patients applied 5-FU 5% cream twice daily for 4 weeks (4)
Treatment failure was defined as clinical evidence of residual tumour, tumour recurrence or progression into an invasive tumour. Tumour presence or keratosis at the site of the initial tumour on first (3 months) follow-up visit following 5-FU or PDT was considered residual tumour. For SE, information on residual lesions was obtained from the pathology report. Recurrence was defined as a new proliferation at the site of the original tumour. In cases of doubt, the suspicion was histopathologically confirmed.
Descriptive results are presented as numbers and percentages for categorical variables and as means (±standard deviation) for continuous variables. The χ2 test and one-way analysis of variance (ANOVA) were used to test differences between treatment groups for statistical significance. Cumulative probability of treatment failure at 1, 2 and 5-years follow-up was calculated with Kaplan–Meier analysis and the log-rank test was used for comparison between treatments. Follow-up ended at the date of diagnosis of treatment failure or at the date of last follow-up visit. Cox regression analysis was performed to calculate hazard ratios (HR) with 95% confidence intervals (95% CI) using SE as the reference group. Variables coding for relevant baseline characteristics (age, sex, lesion diameter, tumour localization and use of immunosuppressive medication) were entered as independent variables to adjust for potential confounding due to differences in baseline characteristics between treatment groups. Missing values on tumour diameter were dealt with using multiple imputation techniques. p-values ≤ 0.05 were considered to indicate statistical significance. Data analyses were performed with SPSS 23.0 (IBM Corp., Armonk, NY, USA) and Stata Version 14 (Stata Corp, College Station, TX, USA).
A total of 1,688 histological reports on BD were identified. Of those, 847 cases were excluded (Fig. S1).
A total of 841 tumours in 608 patients were included. Baseline characteristics are shown in Table SI. Most patients were treated with either SE (n = 296) or PDT (n = 241). 5-FU was used in 46 patients. The majority of patients (78.6%) had only one BD. Median follow-up was 18 months (range 0–87 months).
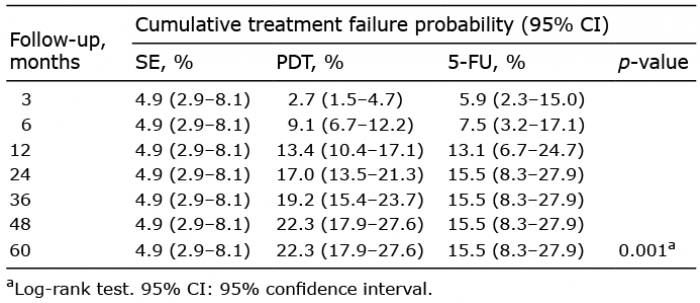
Cumulative probabilities of treatment failure are summarized in Table I. The number of recurrences following 5-FU remained more or less stable after one year, whereas recurrences post-PDT developed even after 3 years. Crude and adjusted hazard ratios (HRs) for PDT and 5-FU compared with SE are summarized in Table SII. After adjustment for differences in baseline characteristics between the treatment groups, PDT is associated with a significantly higher risk of treatment failure than SE (HR 2.71 with 95% CI: 1.52–4.83). 5-FU also showed increased risk compared with SE (adjusted HR 2.22, 95% CI: 0.98–5.04). A slightly higher, statistically non-significant, risk was found for PDT compared with 5-FU (adjusted HR 1.22, 95% CI: 0.62–2.41).
Table I. Cumulative probability of treatment failure after surgical excision (SE) vs. photodynamic therapy (PDT) vs. 5-fluorouracil (5-FU), based on Kaplan–Meier survival analysis
Of all treated BD (n = 841), 8 tumours (< 1%) progressed into an invasive SCC 3–42 months post-treatment. Seven SCCs (2.4%) occurred in patients post-PDT and one (2.1%) after 5-FU.
The results of this study show that BD treated with 5-FU and PDT have a more than 2-fold increased 5-year probability of treatment failure compared with SE, whereas there is no statistically significant difference between 5-FU and PDT. Only a small percentage of the tumours treated with non-invasive therapy progressed into an invasive SCC.
A systematic review assessed the different therapies for BD, including 9 studies: PDT and 5-FU appeared effective, but due to limited evidence no firm conclusions on comparative efficacy were made (7). SE was not included, because of an absence of comparative studies. Morton et al. (10) showed estimated complete response rates of 80% for MAL-PDT (n = 96) and 69% for 5-FU (n = 30) after 12 months’ follow-up. Salim et al. (11) demonstrated a significantly better efficacy of ALA-PDT (82%) compared with 5-FU (48%) in 66 BD in 40 patients. SE showed the lowest recurrence rates of 0.8–5.5% (3, 12).
In our study population, 8 tumours progressed into a SCC after non-invasive therapies. SCCs following complete excision were not observed, but we did find 18 SCCs in the excision specimen that were diagnosed as BD on biopsy. These cases were excluded from further analysis. This finding may indicate that BD lesions treated with SE represent a group with higher clinical suspicion of SCC, which treating physicians consider as unsuitable for treatment with non-invasive modalities. Invasive progression of 2.3–12.6% is reported in the literature after treatment with excision, cryotherapy or PDT (12, 13).
We found differences in onset of treatment failure occurrence, especially with PDT-treated tumours still developing recurrences after 3 years. Late recurrences have also been observed following treatment of sBCC, and this underlines the need for long-term follow-up after treatment with non-invasive therapies (14).
Although SE is associated with a lower probability of treatment failure, non-invasive therapies can be considered an option for tumours at sites with poor/delayed wound-healing and in case of large/multiple tumours (4–6). Differences in cosmetic results, patient preferences and costs should be taken into account when choosing a therapy. Patients should be informed about all aspects in order to make a conscious shared decision.
Because of the non-randomized design, bias due to confounding by indication cannot be ruled out. We attempted to minimize this bias by adjustment for differences in baseline characteristics, but it is possible that not all relevant determinants were captured in the multivariable Cox regression model. Because of the retrospective nature of the study, information on the photosensitizer used could not be retrieved; therefore separate analyses for ALA- vs. MAL-PDT were not possible.
In conclusion, this study showed that SE is associated with the lowest probability of treatment failure in the management of BD. No significant difference between 5-FU and PDT was found, up to 5-years post-treatment.
Conflicts of interest: NWJK-S and MHEJ both report non-financial support (congress) for a presentation from Galderma (February 2017) outside the submitted work.


 Click to show fullsize
Click to show fullsize