


Department of Dermatology, Kyungpook National University School of Medicine, 130, Dongduk-ro, Jung-gu, Daegu, Republic of Korea. *E-mail: yhjang@knu.ac.kr
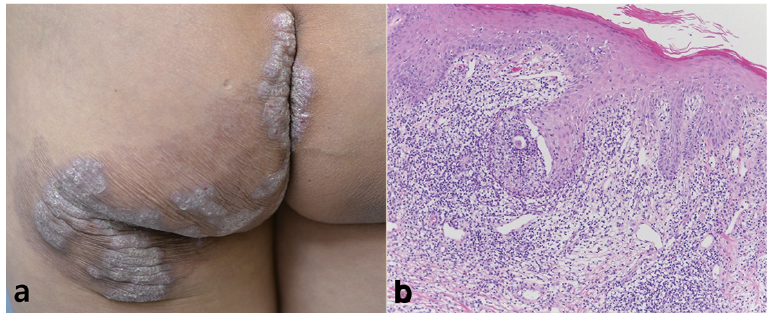
A 43-year-old Asian woman presented to our clinic with mildly pruritic hyperkeratotic and verrucous erythematous plaques and peripherally hyperpigmented patches on the left buttock and intergluteal cleft (Fig. 1a). She reported onset of the skin lesions occurring approximately 20 years earlier. The lesions had gradually increased in size and thickness, accompanied by mild pruritus. There was no improvement on treatment with oral medication, including several years’ treatment with corticosteroid and antihistamine. Her personal and family medical histories were unremarkable. Physical examination was normal, with no evidence of lym-phadenopathy. Complete blood cell count, C-reactive protein level, and erythrocyte sedimentation rate were also normal. Serologies for human immunode?ciency virus, sy-philis, and hepatitis virus were negative. Chest radiography and KOH examination of the skin lesion showed non-specific results. Histopathological examination of the plaques revealed acanthosis in the epidermis, dense inflammatory cell infiltration consisting of neutrophils, lymphocytes, and perivascular infiltration in the superficial dermis (Fig. 1b).
Fig. 1. (a) Hyperkeratotic erythematous plaques and peripherally hyperpigmented patches on the left buttock and intergluteal cleft.(b) Irregular acanthosis and dense lymphohistiocytic infiltration with granulomatous inflammation (hematoxylin and eosin (H&E) staining, original magnification × 100).
What is your diagnosis? See next page for answer.
Acta Derm Venereol 2017; XX: XX–XX.
Diagnosis: Tuberculosis verrucosa cutis
Chronic granulomatous inflammation with many giant cells was observed in the mid-dermis (Fig. 2a). For the skin biopsy specimen, Ziehl-Neelsen staining, tissue culture, and real-time PCR for Mycobacterium tuberculosis were performed, all with negative results. However, positive results were obtained from interferon-gamma release assays (IGRAs; QuantiFERON-Tbc Gold In-Tube test). Subsequent treatment with 3 tablets of fixed-dose combination formulation, including isoniazid 75 mg, pyrazinamide 400 mg, rifampicin 150 mg, and ethambutol hydrochloride 275 mg, was prescribed once a day for the skin lesions. Complete resolution of the plaques was observed after 5 months of treatment. The previous skin lesions showed only asymptomatic hyperpigmentation with no recurrence of disease (Fig. 2b).
Fig. 2. (a) Granulomatous infiltration throughout the dermis with giant cells in the mid dermis (H&E staining, original magnification × 200). (b) Completely resolved hyperkeratotic plaques after 5 months of treatment.
Tuberculosis verrucosa cutis (TVC) is a cutaneous tuberculosis (Tbc) and paucibacillary form caused by exogenous re-infection in previously sensitized individuals (1). TVC is rare in Western countries, but more frequent in Asia. TVC commonly occurs on the hands in adults but has a predilection for the lower extremities in children (2, 3). In Europe, the lesions are reported to present most commonly on the hands, although the lower limbs and buttocks are the more frequently reported sites in Eastern countries (4). The lesions are typically asymptomatic and start as small papules or papulo-pustules, slowly progressing to verrucous or hyperkeratotic plaques. The plaques are firm, and the verrucous surfaces sometimes have fissures and may discharge pus. Regional lymph nodes are not usually enlarged (2).
Diagnosis of TVC is challenging and requires correlation of clinical, histological, and laboratory findings, and diagnostic test results. Histological features are characterized by prominent pseudoepitheliomatous hyperplasia of the epidermis with hyperkeratosis and dense inflammatory cell infiltration composed of neutrophils, lymphocytes, and giant cells. Typical cutaneous Tbc foci show granulomatous infiltration, but caseous necrosis is uncommon (2, 5). The positivity rates in acid-fast bacilli culture and DNA PCR, and detection of M. tuberculosis in Ziehl-Neelsen stain are relatively low because the bacillary load in cutaneous Tbc is less than that in other forms of Tbc (6). IGRA is used as a good diagnostic aid in obtaining detective evidence of M. tuberculosis in TVC (7). Moreover, remarkable response to anti-Tbc therapy might be useful as a diagnostic criterion (5).
The management of cutaneous Tbc follows the same guidelines as that of Tbc of other organs (8). Conventional anti-Tbc therapy is not only used to show improvement of the skin lesions but can also be an essential component of the diagnosis. Thus, successful response to treatment over a period of 6 weeks should be conducive to making a diagnosis (5).
In conclusion, to consider cutaneous Tbc, which can be localized on any part of the body, the chronic verrucous hyperkeratotic plaques should be unresponsive to empirical treatment.


 Click to show fullsize
Click to show fullsize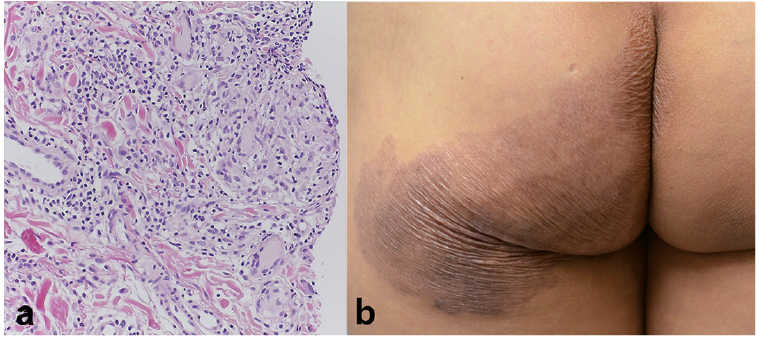 Click to show fullsize
Click to show fullsize