


1Department of Dermatology, and 2Department of Radiation Oncology, Martin Luther University Halle-Wittenberg, Halle (Saale), Germany
In recent analyses of Merkel cell carcinoma, prognosis is poor even in stages I and II. We performed a monocentric retrospective study of 37 consecutive cases with Merkel cell carcinoma stage I to III treated with a combination of surgery and adjuvant radiation to evaluate progression-free and overall survival. The median primary tumour diameter was 17.9 mm. Cases consisted of 31 primary tumours, of which 13 had negative sentinel lymph node biopsy (IA n = 10 and IIA n = 3) and 18 no sentinel lymph node biopsy (IB n = 15 and IIB n = 3), 2 tumours with positive sentinel lymph node biopsy (IIIA) and 4 with local macrometastasis (IIIB). The median age was 71 years and the median follow-up was 60.4 months. The 5-year progression-free survival was 83.8% and 5-year disease-specific survival was 95.7% (overall survival 93.0%). So far, our results show a high survival rate with combined treatment of surgery and adjuvant radiotherapy in early tumour stages of Merkel cell carcinoma.
In literature Merkel cell carcinoma is depicted as a rare but aggressive and metastasizing skin tumour. Our results of 37 consecutive patients treated by combined surgery and adjuvant radiotherapy show a low regional recurrence rate as well as a high 5-year disease-specific survival rate (95.7%). The combination of surgery and adjuvant radiotherapy may improve the management of localized MCC with or without limited involvement of loco regional lymph nodes. Because of the discrepancy between the effects of combined therapy versus surgery alone systemic therapies could also be considered if due to contraindication to RT a combined therapy is impossible.
Key words: Merkel cell carcinoma; MCC; combined treatment; adjuvant radiotherapy.
Accepted Jan 29, 2018, Epub ahead of print Jan 30, 2018
Acta Derm Venereol
Corr: Eckhard Fiedler, MD, Department of Dermatology, Martin Luther University Halle-Wittenberg, Ernst-Grube-Straße 40, DE-06120 Halle (Saale), Germany. E-mail: eckhard.fiedler@halle-hautarzt.de
In the literature, Merkel cell carcinoma (MCC) is described as an aggressive metastasizing neuroendocrine skin tumour. In current papers, high mortality rates are reported even in low tumour stages (1, 2). A 5-year overall survival (OS) rate of 64% is reported for localized tumours (stage I and II), and 39% for loco-regional lymph node metastases (stage III) (2). Beside excision with wide margins, adjuvant radio-therapy (RT) of the primary tumour site and regional lymph node bed in early tumour stages has been widely recommended for more than 20 years (3), though it still remains controversial (4). The question of suitable tumour stages for systemic approaches arises in light of new therapeutic strategies, including PD1 inhibitors (2, 5).
This research is a retrospective monocentric study of consecutive patients with MCC who were treated with excision and adjuvant RT and followed up at the Department of Dermatology of the Martin Luther University Halle-Wittenberg from 2000 to 2017.
Between 2000 and 2017, 41 consecutive patients with histologically and immunohistologically-confirmed diagnosis of MCC came for therapy and follow-up care to the Department of Dermatology.
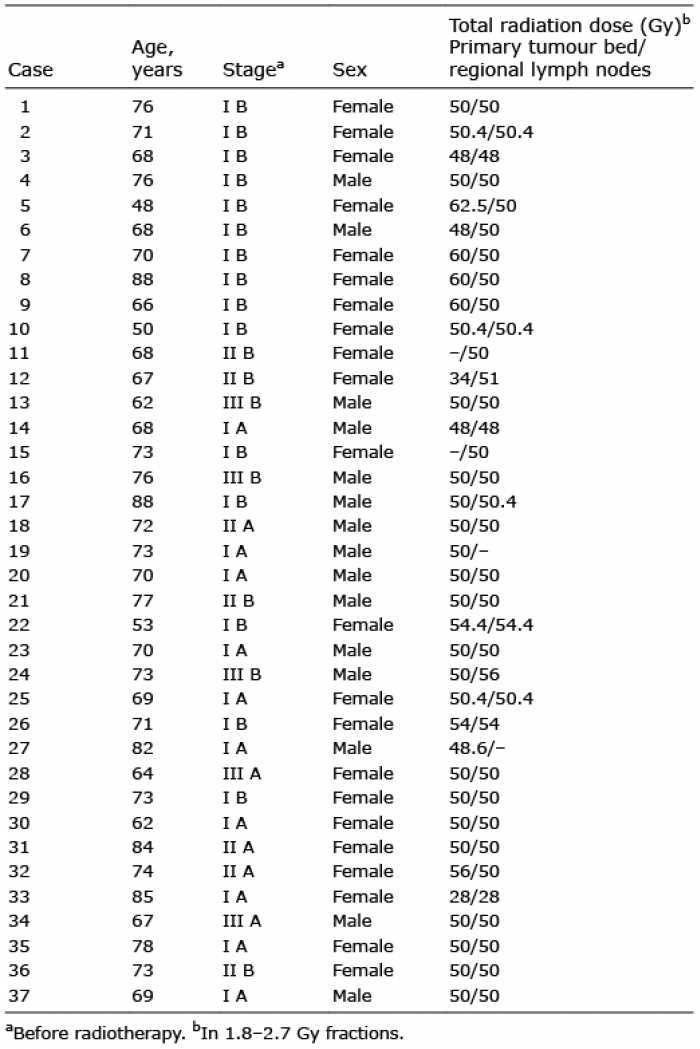
If there was neither contraindication nor refusal of treatment, an R0-resection – if possible with wide excision margins – and adjuvant RT of the primary tumour site and regional lymph node bed were performed. Doses of 48 to 60 Gy were used. Due to side effects of radiotherapy 2 patients received 28 Gy and 34 Gy only. After therapy, the patients were transferred to regular follow-up.
Sentinel lymph node biopsy (SLNB) was performed in 13 patients (35.1%). The median excision margin was dependent on the location of the primary tumour site: limbs 18 mm (n = 24; range 0.1–30), head and neck 10 mm (n = 11; range 1.0–20), and trunk 20 mm (n = 2; range 20.0/20.0). The median excision margin was 10 mm in all 37 cases. Cases with primary distant metastases (stage IV) or inoperable bulky disease were excluded, as were cases in which the patient refused combined treatment (excision and RT). Ten-year follow-up included clinical (months 0 to 48: every 3 months, months 48 to 120: every 6 months) and ultra sound examination of primary tumour site and regional lymph nodes (months 0 to 24: every 3 months, months 24 to 60: twice a year, months 60 to 120: once a year), chest X-rays and abdominal ultra sound: months 0 to 120: once a year.
TNM staging was made according to UICC TNM 7th edition (6).
Statistics including Kaplan Meier survival analysis were performed using IBM SPSS statistical software.
Of 41 MCC patients, 3 were in need of systemic therapy (2 stage IV and 1 with bulky metastatic disease (stage III)). Another patient refused radiotherapy. The remaining 37 cases are shown in Table I. The group under observation included 22 women (59.5%) and 15 men (40.5%) (Table II). At the time of radiotherapy, 10 tumours were classified stage IA, 15 stage IB, 3 stage IIA, 3 stage IIB, 2 stage IIIA and 4 stage IIIB (of which 1 was metachronous stage IIIB after stage IIB at first diagnosis) according to UICC TNM 7th edition (6). The median age was 71 years (range 47–88 years).
Table I. Radiotherapy data
Table II. Tumour-specific, demographic and therapeutic data
The limbs comprised the most frequently treated site (64.9%; n = 24), followed by head and neck (29.7%; n = 11) and the trunk (5.4%; n = 2). The median follow-up was 60.4 months (range 0.4 to 199.8 months).
Patients reported a median time span of 3 months (range 0.1–240 months) between first symptoms and primary surgery of the tumour. The median size of the tumour at the time of surgery was 17.9 mm (range 5.0–30.0 mm); 75.7% (28/37) reported horizontal growth. The same percentage observed vertical growth. In 2 cases (5.4%), a change of colour was noticed.
Three tumours (8.1%) were symptomatic with pain. Two (5.4%) had bled. The median time of horizontal growth was 2 months (range 3 days–1 year); vertical growth 2.5 months (range 3 days–1.5 years).
Thirteen of 37 patients (35.1%) used statins. Nine (24.3%) reported a known diabetes mellitus; 1 myasthenia gravis, 2 rheumatoid arthritis (1 using methotrexate). For all 37 cases, the 5-year progression-free survival was 86.5% (mean estimate 155.1 months; 95% confidence interval (CI) 122.4–187.8; standard error [SE] 16.7) (Fig. 1A) and the 5-year disease-specific survival was 95.7% (mean estimate 192.4 months; 95% CI 178.1–206.6; SE 7.3) (Fig. 1B). The 5-year overall survival was 93.0% (mean estimate 163.8 months; 95% CI; 135.8–191.9; SE 14.3) (Fig. 1C).
Fig. 1. (A) Progression-free survival (PFS), (B) disease-specific survival (DSS) (C) Overall survival (OS) and (D) distant metastasis-free survival (DMFS) of 37 Merkel cell carcinoma (MCC) patients (A: 10 stage IA, 15 stage IB, 3 stage IIA, 3 stage IIB, 2 stage IIIA and 4 stage IIIB (of which one was metachronous stage IIIB after stage IIB at first diagnosis). B: 10 stage IA, 15 stage IB, 3 stage IIA, 3 stage IIB, 2 stage IIIA and 4 stage IIIB (of which one was metachronous stage IIIB after stage IIB at first diagnosis. C: 10 stage IA, 15 stage IB, 3 stage IIA, 3 stage IIB, 2 stage IIIA and 4 stage IIIB (of which one was metachronous stage IIIB after stage IIB at first diagnosis. D: (10 stage IA, 15 stage IB, 3 stage IIA, 3 stage IIB, 2 stage IIIA and 4 stage IIIB (of which one was metachronous stage IIIB after stage IIB at first diagnosis)).
The stage IB 5-year progression-free survival was 86.2% (mean estimate 148.8 months; 95% CI 106.9–190.7; SE 21.4) and the stage IB 5-year disease-specific survival was 92.3% (mean estimate 186.7 months; 95% CI 161.9–211.4; SE 12.6).
After completion of treatment, 6 patients (16.2%) developed loco-regional or distant metastases (Table III). The median time span from radiotherapy to first metastasis was 14.7 months (range 2.6–94.3 months). Three patients developed loco-regional metastases 2.6 months, 3.4 months, and 16.7 months after radiotherapy. Of those 3, 2 occurred inside the primary radiation field. Distant metastases were found in 4 cases after median 43.8 months (range 12.1–94.3 months). Two distant metastases were cutaneous only, the other 2 visceral and distant lymph node metastases. The 5-year distant metastasis-free survival was 91.9% (mean estimate 167.1 months; 95% CI 137.5–196.6; SE 15.1) (Fig. 1D).
Table III. Merkel cell carcinoma (MCC) metastases
In our group, only one patient died of progressive MCC disease, 4 of other causes (2 cardiac disease, 1 malignant tumour of different origin, 1 non tumour-related cause).
Secondary tumours and comorbidities are summarized (Tables IV and V).
Table IV. Secondary tumours of different origin before and after Merkel cell carcinoma (MCC) diagnosis
Table V. Comorbidities and other immunosuppressive conditions
Due to the low incidence of MCC, monocentric studies collecting cases over long time periods often contain changes in therapeutic regimens (7). Interesting parameters are often missing in retrospective studies using epidemiologic databases (8, 9). The study at hand is a monocentric retrospective analysis based on a relatively homogenous treatment course.
The tumour stage of MCC is an important predictor of prognosis (10). Early tumour stages (I and II) are the best represented in our study, since combined treatment is adequate here. Eighty-seven percent of regional lymph node involvement occurs within 2 years of diagnosis (11).
Immunosuppression results in worse prognosis in MCC (12). No immunosuppressive drugs were taken by our patients, except one case of methotrexate taken because of rheumatoid arthritis.Conspicuous is a relatively high percentage of diabetics (24.3%) among our patients. 7 cases showed MCC as a secondary cancer of different origin. Five patients developed a different cancer during follow-up (Table IV).
Although not classic immunosuppressive drugs, some immunosuppressive impact is suspected in statins. Statin use is reported as disadvantageous, especially in young patients (13). 35.1% of our patients reported using statins (Table V). The median age of our group of statin users is 72.8 years (range 61.6–84.6 years). Due to the age of these patients, the high percentage of statin users does not seem unusual. No accumulation of negative courses of disease was observed in our group. Another point of interest could be that none of the 29 reported family histories contained MCC in any generation. Typically, MCC is rapid-growth and painless (2). We found a median time span of 3 months (range 0.1–240 months) between the patient’s first symptom and primary surgery of the tumour. 8.1% of our group reported painful nodules. The median size of the primary tumour at the time of surgery was 17.9 mm (range 5.0–30.0 mm), with 67.6% of the cases stage I (IA and IB). RT offers advantages for the head and neck region (14, 15), but less than one-third (29.7%) of our cases had primary tumour sites in that region.
An earlier study found improvement of local control after adjuvant RT but no effect on survival (16). Our results may indicate that adjuvant RT improves not only local control but also progression-free survival in early stages of MCC, especially in stage IB as stated in the literature (17). The 5-year progression-free survival for all 37 cases was 86.5% (median follow-up 60.4 months) and the 5-year disease-specific survival was 95.7%. Due to our study design, all cases underwent radiotherapy, which is why the influence of RT in the therapy of our patients must remain unclear.
One patient out of the 4 who developed distant metastases died due to MCC, the other 3 are still alive (median follow-up since stage IV diagnosis: 36.6 months). Of the 3 living patients, only one was diagnosed with another solitary cutaneous distant metastasis, the others are still without further metastases.
Predictors of worse disease-specific overall survival rate include age older than 75 years, number of lymph nodes involved, tumours larger than 50.0 mm, metastatic disease, or lack of radiation therapy. Of these, the number of involved nodes was the best predictor (18). Our findings support these conclusions in so far as our patients, though elderly, have neither tumour sizes larger than 50 mm nor a larger number of lymph nodes involved, show few metastases and do not lack RT (exclusion criterion) but achieve a high survival rate. These criteria could help to discriminate patients suitable for combined therapy versus patients better treated with other approaches. We conclude that besides the combined therapy, the low median primary tumour size and the low number of immunosuppressive therapies are the main reasons for the good outcome in our cohort.
Güler-Nizam et al. (19) found a 78% tumour-specific 5-year overall survival for stage I MCC and a 100% tumour-specific 2-year overall survival in the group that underwent radiotherapy after excision of the primary tumour. The median age of the reported 57 cases is the same as in our group, but only 9 of the Güler-Nizam cases underwent radiotherapy after excision of the primary lesion (19). A higher proportion of undiscovered positive SLN in the group in whom no SLNB was performed (stage IB and IIB) might be in part responsible for the lower tumour-specific OS compared to our group.
Sentinel lymph node biopsy (SLNB) results are an important tool to estimate the tumour burden and various other risk factors (20). SLNB in MCC is recommended according to German therapy guidelines (21). The main importance of SLNB is better staging (22) and selection of candidates for completion lymph node dissection (CLND) (if SLNB is positive), since adjuvant radiotherapy of regional lymph nodes is reported to be beneficial even if negative SLNB (23, 24).
While 26.7% (lower rate of regional relapses) of stage IB patients developed metastases during follow-up, only 10% of the stage IA patients did. This might be due to the unknown microscopic lymph node status in stage IB.
We used median 10.0 mm excision margins (range 1–30 mm). Other studies show equal results for R0 resection using Mohs surgery and wide-local excision (25). Due to the good radiosensitivity of MCC cells, smaller excision margins are discussed (26). Adjuvant RT improves local control and survival (2). Taken together, our results show a good effect of combined therapy on the early stages of MCC, since the 5-year disease-specific survival was 95.7% in a median follow-up of 60.4 months. Our experience is in line with various papers suggesting the combination of surgery and adjuvant RT as a standard for MCC treatment in early tumour stages (2, 16).
The use of adjuvant RT is viewed differently considering side effects and requirements of the various regions of the body, (27); 50–55 Gy has been suggested as the optimal total dose for head and neck (4). Total doses of 48 to 60 Gy were used for our patients. Because of side effects, 2 RT series were ended early without verifiable negative impact on the course of the disease and survival.
New systemic approaches to therapy, which apply especially to inoperable tumours, should be measured against the combination of surgery and RT as a standard in potentially treatable MCC (stages I to III). Because of the discrepancy between the effects of combined therapy versus surgery alone, systemic therapies could also be considered if combined therapy is impossible due to RT contraindication.
Larger studies on adjuvant therapy in early stages of MCC are necessary to compare the prospect of success, because the described effects on survival in smaller studies differ even when the same treatment is applied.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize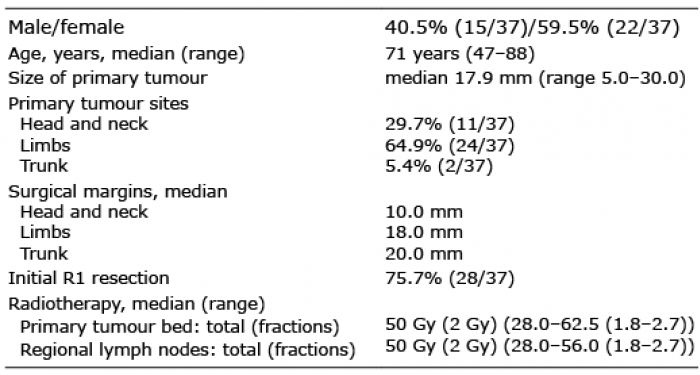 Click to show fullsize
Click to show fullsize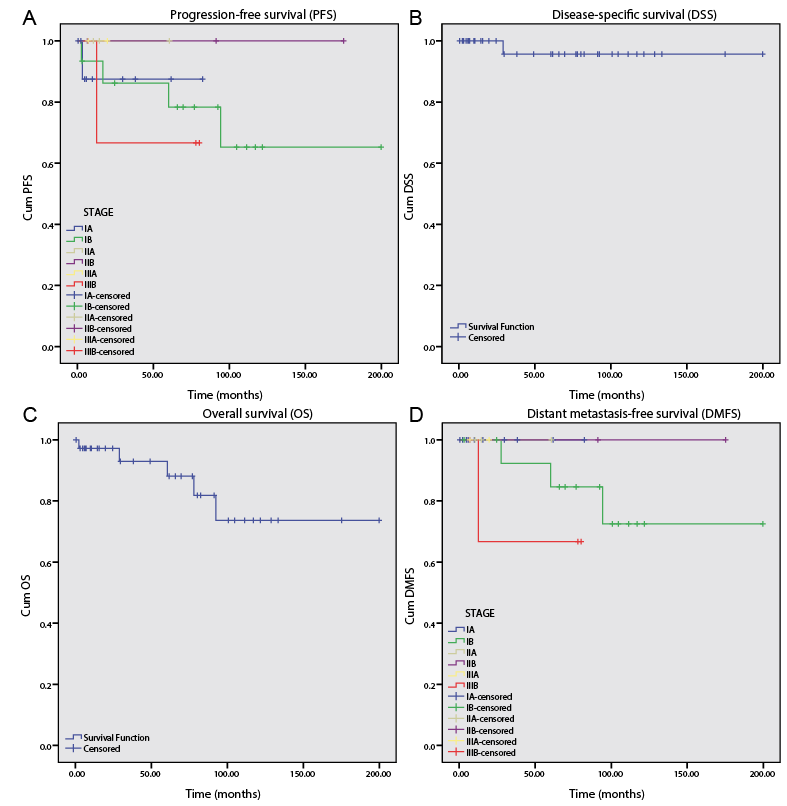 Click to show fullsize
Click to show fullsize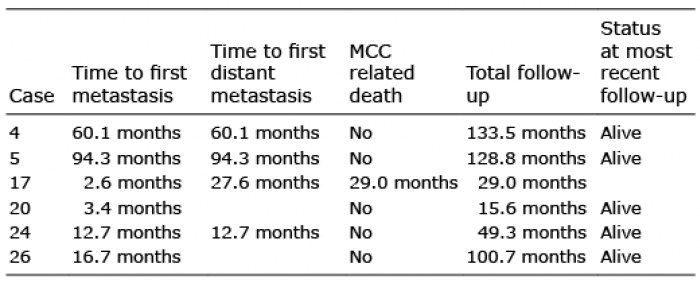 Click to show fullsize
Click to show fullsize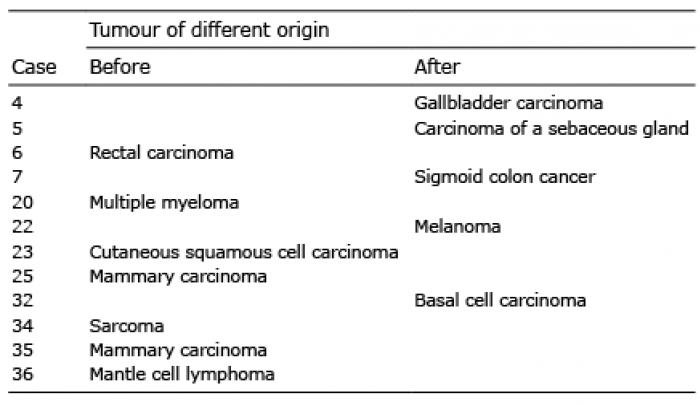 Click to show fullsize
Click to show fullsize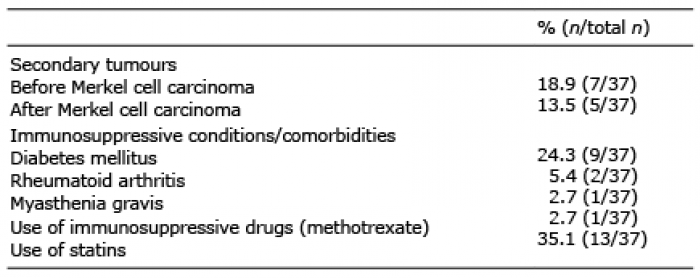 Click to show fullsize
Click to show fullsize