


1Skåne University Hospital, Malmö, 2Department of Medical and Health Sciences, Linköping University, Linköping, Sweden, and 3LEO Pharma A/S, Ballerup, Denmark
Psoriasis is a chronic inflammatory disorder that imposes a substantial economic burden. We conducted a cost-utility analysis from a Swedish healthcare payer’s perspective using a decision-tree model with a 12-week time horizon. Patients with psoriasis vulgaris could have two 4-week cycles of topical treatment with calcipotriol 50 µg/g and betamethasone 0.5 mg/g as dipropionate (Cal/BD) foam or Cal/BD ointment before progressing to phototherapy/methotrexate. In the base-case analysis, Cal/BD foam dominated over Cal/BD ointment. The increased efficacy of Cal/BD foam resulted in fewer consultations and a decreased risk of progressing to phototherapy/methotrexate. Although Cal/BD foam costs more than Cal/BD ointment, this was offset by lower costs for phototherapy/methotrexate or consultation visits. Sensitivity analyses revealed that the base-case net monetary benefit was robust to plausible variations in key parameters. In conclusion, Cal/BD foam was predicted to be more cost-effective than Cal/BD ointment in the treatment of psoriasis vulgaris.
Key words: psoriasis; cost-utility analysis; calcipotriol; betamethasone dipropionate.
Accepted Jan 7, 2019; E-published Jan 9, 2019
Acta Derm Venereol 2019; 99:
Corr: Lasse Ryttig, LEO Pharma A/S, DK-2750 Ballerup, Denmark. E-mail: lgydk@leo-pharma.com
Psoriasis is a chronic heterogenous disorder with a substantial impact on patients and healthcare systems. We evaluated the cost-effectiveness of Cal/BD foam versus Cal/BD ointment over a 12-week time horizon in patients with psoriasis, from a Swedish healthcare perspective. In our model, the superior efficacy of Cal/BD foam over ointment led to fewer consultation visits, a decreased risk of progressing to second-line therapy, and lower total costs. Improved topical therapies, such as Cal/BD foam, have the potential to reduce the need for some patients to progress to phototherapy and/or systemic treatment, which may lead to a reduction in the overall treatment costs of psoriasis.
Psoriasis is a chronic inflammatory disorder with a prevalence of 4–9% in Northern Europe (1). It is a chronic and heterogeneous disease with an unpredictable course and progression (2), which often does not follow a progressive course but rather a periodic pattern of remissions and flare-ups. Psoriasis has a significant detrimental impact on patients’ health-related quality of life, as well as imposing a substantial economic burden on society (3, 4).
Topical treatment is often sufficient in patients with mild-to-moderate psoriasis (5), with combined topical therapy with a vitamin D analogue and a corticosteroid shown to have greater efficacy than any single component alone (6). Systemic treatment (e.g. methotrexate) or phototherapy may be indicated in patients who do not respond to the first-line topical therapy (5). Methotrexate is the most commonly prescribed systemic agent for psoriasis in Sweden (7).
Ointment, gel and aerosol foam formulations with a fixed combination of calcipotriol 50 µg/g and betamethasone 0.5 mg/g as dipropionate (Cal/BD) are available for the topical treatment of adults with psoriasis vulgaris (8, 9). Previous European cost-effectiveness analyses have shown that Cal/BD ointment or gel is more cost-effective compared with monotherapy with Cal or BD (or another potent corticosteroid) (10–12), morning application of Cal and evening application of BD (or another potent corticosteroid) (10, 11, 13, 14) or other topical therapies (11–13, 15).
The clinical efficacy of Cal/BD aerosol foam formulation (Enstilar®) in patients with psoriasis vulgaris was established in Phase II and III trials. In Phase II trials, significantly (p < 0.05) higher treatment success rates (assessed using the Physician Global Assessment [PGA] of disease severity, a 5-point severity scale [‘clear’, ‘almost clear’, ‘mild’, ‘moderate’, ‘severe’]) were seen with Cal/BD foam than with Cal foam or BD foam alone (NCT01536938) (16) or with Cal/BD ointment (NCT01536886) (17). In Phase III trials, patients using Cal/BD foam experienced significantly (p < 0.001) higher treatment success rates (assessed using PGA) than patients using vehicle (PSO-FAST study; NCT01866163) (18) or Cal/BD gel (PSO-ABLE study; NCT02132936) (19). In these Phase III trials, significantly (p < 0.001) more patients using Cal/BD foam than vehicle achieved a 50% or 75% reduction in the Psoriasis Area and Severity Index (PASI50 or PASI75) (18), and significantly (p < 0.01) more patients using Cal/BD foam than Cal/BD gel achieved PASI75 or a 90% reduction in PASI (19). Patient preference is affected by many factors, such as efficacy. Additional factors include the choice of vehicle, and because of the greasiness of the ointment, foam is generally considered significantly more convenient by patients (20–22).
We conducted this pharmaco-economic analysis to evaluate the cost-effectiveness of Cal/BD foam versus Cal/BD ointment (Daivobet®) in patients with psoriasis vulgaris from the perspective of the Swedish healthcare system in a short-term decision-making context. This evaluation is comparing flare treatment with two topical treatments for 12 weeks.
A cost-utility analysis was conducted to evaluate the incremental cost per quality-adjusted life year (QALY) gained from Cal/BD foam versus Cal/BD ointment in patients with psoriasis vulgaris. The analysis was conducted from the Swedish healthcare payers perspective and used a decision-tree model. The model had a 12-week time horizon comprising three cycles of 4 weeks’ duration each, corresponding to the 4-week treatment period recommended in the Cal/BD foam and Cal/BD ointment summary of product characteristics (SmPC) (8, 9). Based on the expert advice, patients could have two 4-week cycles of topical treatment plus an additional 4 weeks to evaluate the treatment effect and determine whether second-line therapy was needed. Discounting of outcomes and costs was not applied because of the 12-week time horizon. A Swedish expert panel comprising of two expert dermatologists in psoriasis and two health economists validated the model.
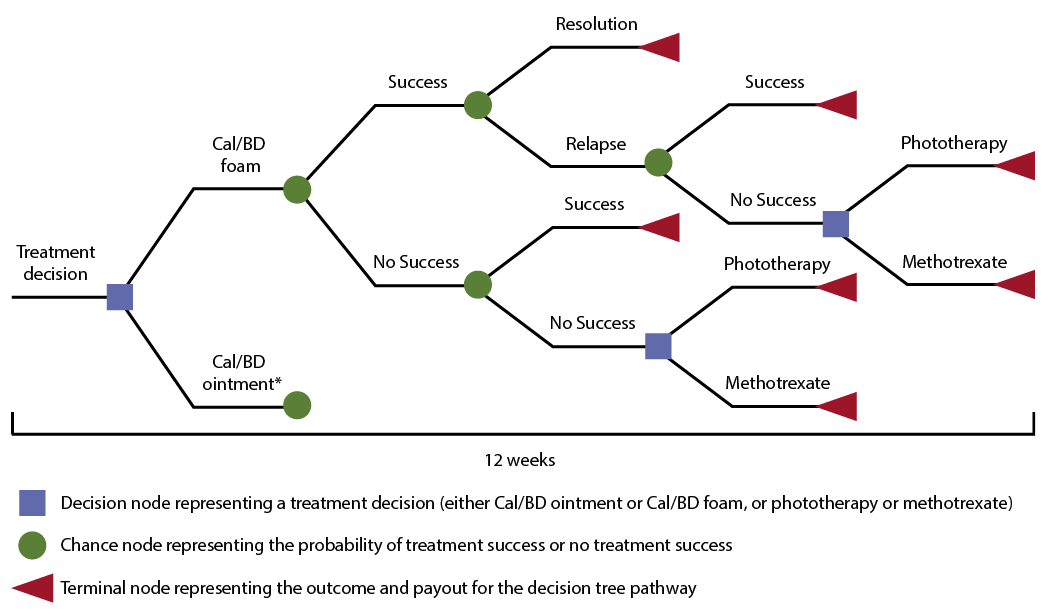
The decision-tree model was developed using Microsoft Excel® 2010 (Fig. 1). Upon entering the model, all patients were initially treated with Cal/BD foam or Cal/BD ointment once daily for 4 weeks, with the possibility of receiving one more treatment cycle with the same topical treatment. At the end of the cycle, patients could have achieved either treatment success (responder) or no treatment success (non-responder). Responders could either stay in remission for the remaining 8 weeks or experience a relapse, in which case they would have an additional general practitioner (GP) visit and initiate a second course of the topical treatment they started with. A relapse followed by a non-response would result in referral to a specialist, and initiation of either phototherapy or methotrexate. Patients with no treatment success after 4 weeks (non-responders) had an additional GP consultation to initiate a second course of the original topical therapy. The treatment dose, regimen and probability of treatment success were assumed to be the same as for the initial 4-week treatment period. If the second round of treatment was not successful, the patient progressed to the next level of treatment with a visit to a specialist and initiation of either phototherapy or methotrexate.
Fig. 1. Structure of the decision tree. *Although not shown, the decision tree structure for the calcipotriol 50 µg/g and betamethasone 0.5 mg/g as dipropionate (Cal/BD) ointment arm is the same as for the Cal/BD foam arm. Following 4 weeks’ treatment with Cal/BD foam or Cal/BD ointment, patients achieved either success (responders) or no success (non-responders). Responders could then stay in remission for the remaining 8 weeks (resolution) or experience a relapse, in which case they initiated a second 4-week course of the topical treatment they started on. A relapse followed by non-response resulted in initiation of phototherapy or methotrexate. Non-responders initiated a second course of the original topical therapy; if this was not successful, either phototherapy or methotrexate was initiated.
We considered a hypothetical adult population of patients with psoriasis vulgaris who were candidates for the topical treatment.
We selected Cal/BD ointment as the most relevant comparator for comparison with Cal/BD foam – a choice that was confirmed by Swedish clinical experts on psoriasis and accepted by the Swedish Dental and Pharmaceutical Benefits Agency (TLV). Both Cal/BD foam and Cal/BD ointment have the same approved indication and duration of treatment (8, 9), with Cal/BD ointment being fully reimbursed and the most frequently prescribed fixed combination Cal/BD topical treatment in Sweden in 2015 (23).
Clinical efficacy data were obtained from the investigator-blinded, multicenter, Phase II, 4-week trial, directly comparing Cal/BD foam with Cal/BD ointment in which 376 patients with psoriasis vulgaris were randomized to receive Cal/BD foam (n = 141), Cal/BD ointment (n = 135), foam vehicle (n = 49) or ointment vehicle (n = 51) (17). In the study, significantly more patients receiving Cal/BD foam than Cal/BD ointment achieved treatment success at 4 weeks (54.6% vs 43.0%; odds ratio 1.7, 95% CI 1.1, 2.8; p = 0.025; primary endpoint) (17). Treatment success was defined as achieving ‘clear’ or ‘almost clear’ skin with at least a two-step improvement, according to the PGA (17).
These treatment success rates were used for the probability of response values (i.e. 54.6% for Cal/BD foam and 43.0% for Cal/BD ointment) in the base-case model. Other base-case model inputs included a 20% probability of relapse at 4 weeks for all topical agents (based on a Scottish cost-effectiveness analysis (10) and subsequently confirmed by expert opinion), and an 80% probability that the second-line treatment would be phototherapy and a 20% probability that the second-line treatment would be methotrexate (based on expert opinion). Given the short time horizon of 12 weeks for the model, we did not consider the efficacy of second-line treatment.
Local data sources were used to calculate costs and are presented in Table I.
The quantities of Cal/BD foam and Cal/BD ointment used were derived from the Phase II head-to-head study (17).
Use of an 8-week phototherapy treatment duration was based on Medical Products Agency psoriasis guidelines (24) and confirmed by Swedish clinical experts on psoriasis. The 12-week duration of methotrexate therapy was based on the SmPC (25) and the opinion of Swedish clinical experts, and the dosing regimen and monitoring procedures for methotrexate were confirmed by Swedish clinical experts.
Prior to initiating a new round of topical or second-line (phototherapy or methotrexate) treatment, the patient had a consultation with either a GP or a dermatology specialist.
Costs associated with adverse events were not included in the model, as a similar safety and tolerability profile was observed between Cal/BD foam and Cal/BD ointment in the incidence or type of adverse events in the head-to-head trial (17).
Table I. Costs included in the model
No utility data (EuroQol five-dimensions; EQ-5D) were collected in the Phase II trial comparing Cal/BD foam and Cal/BD ointment (17). Hence, the best source of utility was the PSO-ABLE study, a Phase III trial conducted in France, the USA and the UK, which compared Cal/BD foam with Cal/BD gel (19).
A post hoc analysis of PSO-ABLE was performed based on PGA responders and non-responders, as this was not part of the original analysis plan. Based on the 67 PGA responders and the 107 non-responders in the Cal/BD foam study arm, mean EQ-5D utility values were 0.80 at baseline, 0.91 in patients with treatment success (responders) at week 4 and 0.88 in patients without treatment success (non-responders) at week 4. No statistical test was performed on the difference.
Given the time frame of the model, patients incurred the utility of a non-response (0.88) when they received phototherapy or methotrexate. This assumption was tested in a sensitivity analysis.
Base-case analyses evaluated the incremental cost per QALY gained from Cal/BD foam versus Cal/BD ointment, and the net monetary benefit. Net monetary benefit represents the value of an intervention in monetary terms at a fixed willingness-to-pay (WTP) threshold.
Two-way sensitivity analyses were performed focusing on parameters that were likely to alter the cost-effectiveness result (Table II).
All costs were varied by ± 25%. As these are all point estimates, no standard range is available and 25% was chosen as a common range. As phototherapy is a labour-intensive treatment, the cost of which has only increased over the past years and is not expected to decrease, a 25% reduction is therefore considered a conservative estimate. This is also true for the cost of GP and specialist visits. Generics are available for methotrexate tablets and pens, and hence no further significant reductions are expected.
Utilities were varied by ± 2% because of the proximity of the base-case utility values in responders versus non-responders, and the fact that base-case utility values were at the high end of the scale.
Utilization of phototherapy and methotrexate was varied, consisting of 50% phototherapy and 50% methotrexate. The base-case values of 80% phototherapy and 20% methotrexate were based on expert opinion. Expert opinion suggested the lowest plausible range to consider would be 50%/50%.
The rate of relapse was varied by ± 25%. The original rate of 20% was based on an assumption made in another published cost-effectiveness analysis (10), whereas a later study found a 4-week relapse rate of 23.7% (calculated based on the 8-week relapse rate of 41.2%) (26), hence the range of ± 25% was considered sufficient.
Efficacy was varied using different outcome measures. The primary outcome was PGA response, and sensitivity analyses were done on the PASI score for PASI50 and PASI75. The PASI score was chosen based on its relevance as an outcome measure in psoriasis.
Probabilistic sensitivity analyses were also performed. For efficacy measures and utilities, inverse-beta distributions were applied. Standard deviations (SDs) were taken from the clinical trial reports. For the relapse rate, an inverse-beta distribution was also applied, but here only the point estimate was available and hence we applied a 25% SD to the mean as discussed above. For all dosage and costs, inverse-gamma distributions were applied. SDs for the dosages were taken from the trial reports and a 25% SD was applied for the cost.
Table II. Values used in two-way sensitivity analyses
In the base-case analysis, Cal/BD foam was associated with an incremental QALY gain of 0.0008 and lower total costs (−SEK2,419), meaning Cal/BD foam dominated over Cal/BD ointment (i.e. was more effective for the treatment of psoriasis and less costly; Table III). The increased efficacy of Cal/BD foam resulted in fewer GP and specialist consultations, and a decreased risk of progressing to the second-line treatment (phototherapy or methotrexate). This led to lower costs for phototherapy or methotrexate (reflecting lower use) and lower costs for consultation visits (due to fewer consultations) for patients treated with Cal/BD foam than Cal/BD ointment (Table IV). This offset the higher medication cost of Cal/BD foam than Cal/BD ointment, leading to lower total cost of treatment of SEK9,411 (€945) for Cal/BD foam versus SEK11,830 (€1,188) for Cal/BD ointment (difference −SEK2,419; –€243).
Table III. Cost-effectiveness of Cal/BD foam versus Cal/BD ointment: base-case analysis
Table IV. Breakdown of costs (SEK)
The base-case net monetary benefit of Cal/BD foam versus Cal/BD ointment was SEK2,799 (Table V). This positive net monetary benefit indicates that Cal/BD foam is cost-effective versus Cal/BD ointment at a WTP threshold of SEK500,000 (27).
Table V. NMB of Cal/BD foam versus Cal/BD ointment: base-case analysis
Sensitivity analyses found that increasing the utility value for those patients who received methotrexate and phototherapy from non-response (0.88) to the level of responders (0.91) resulted in a reduction in the difference between Cal/BD foam and Cal/BD ointment in incremental QALYs gained (0.0005); however, Cal/BD foam remained the dominant treatment.
Two-way sensitivity analyses revealed that the base-case net monetary benefit (SEK2,799) was robust to plausible variations in key parameters (net monetary benefit ranged from SEK464 to SEK3,528), with Cal/BD foam remaining dominant over Cal/BD ointment (Fig. 2). Although net monetary benefit was most sensitive to a change in the efficacy parameter (i.e. if treatment success was based on the proportion of patients achieving PASI50 rather than PGA response), changing the efficacy parameter from PGA to PASI75 and PASI50 did not change the outcome of the model. Changes in the price of methotrexate tablets or injection pens or in utility weights had very little impact on the results.
Fig. 2. Two-way sensitivity analysis: net monetary benefit. aNet monetary benefit of SEK464; bNet monetary benefit of SEK1,865; cNet monetary benefit of SEK1,880. Cal/BD: calcipotriol 50 µg/g and betamethasone 0.5 mg/g as dipropionate; PASI: Psoriasis Area and Severity Index; PGA: Physician Global Assessment; SEK: Swedish kronor (100 SEK = 9.96 € February 2018).
Probabilistic sensitivity analysis demonstrated that Cal/BD foam remained dominant over Cal/BD ointment in 77% of simulations (Fig. 3).
There was a > 84% probability of Cal/BD foam being considered cost-effective, regardless of the WTP threshold.
Fig. 3. Incremental cost-effectiveness over 1,000 simulations. SEK: Swedish kronor (100 SEK = 9.96 € February 2018).
In this cost-utility analysis conducted from the Swedish healthcare perspective, Cal/BD foam dominated over Cal/BD ointment in patients with psoriasis vulgaris, providing greater efficacy at a lower cost. The increased efficacy of Cal/BD foam resulted in fewer GP and specialist consultations, and a decreased risk of progressing in the treatment pathway and thus requiring second-line therapy (e.g. phototherapy or methotrexate). Cal/BD ointment is an appropriate analogy, as accepted by the TLV, as it has the same approved indication and duration of treatment as Cal/BD foam (8, 9), is fully reimbursed, and was the most frequently prescribed fixed combination Cal/BD topical treatment in Sweden in 2015 (23). The results of this cost-effectiveness analysis are aligned with a recent cost-effectiveness analysis conducted from an Australian healthcare payer perspective, which found Cal/BD foam to be more cost-effective, compared with Cal/BD gel, in patients with psoriasis vulgaris, with an incremental cost per QALY gained of $AUD13,609 (approximately €8,500 or SEK89,000; 2018 values) (28).
Both Cal/BD ointment and Cal/BD foam are indicated for the treatment of mild-to-severe psoriasis. The response definition of a two-step improvement in PGA is a US FDA requirement for treatment response, but PASI response is typically also obtained in psoriasis trials and generally considered the most relevant efficacy measure. Changing the primary efficacy parameter from PGA to PASI75 and PASI50 did not change the outcome of the model. The model requires two attempts of topical treatment before patients can progress to the next line of treatment. Although the response requirement is arguably more arbitrary in real-world treatment practice, this is the response required by authorities and applied in many economic models (29, 30). Patients who fail on topical treatment are eligible for the next line of therapy.
It is worth noting that a conservative approach was taken when estimating the utility values of responders versus non-responders in this cost-utility analysis. This reflects the strict response criteria and the fact that many patients who do not respond according to the criteria will still have significant treatment benefit and hence significant improvement in the utility score. To demonstrate the true impact of the treatment effect, it has been argued that the non-response utility value should be based on non-responders in the vehicle arm.
Strengths of the model used in this analysis are the inclusion of the efficacy data from a head-to-head trial (17) in the base-case analysis, and the capturing of costs associated with second-line systemic therapy or photo-therapy.
A key limitation of the model is the narrow time horizon of 12 weeks. As psoriasis is a chronic disease, it could be argued that the use of long-term models with a time horizon of >1 year would be beneficial to consider how patients progress through the various lines of treatment from topical treatments to phototherapy, immunosuppressants and biologics to best supportive care, considering the costs and efficacies of all products across the entire time horizon. For the purpose of the current decision analysis, it was decided to keep the time horizon to 12 weeks, which was considered sufficient to capture the relevant information, i.e. the efficacy and cost of the two comparator products and the downstream cost of the next line of treatment for patients who failed treatment. In this context, we do not consider the efficacy of photo-therapy or methotrexate, or the topical treatments beyond the 12 weeks. As the efficacy of phototherapy is likely to be higher than the topical treatments and may last longer, this could skew the results in favour of the most efficacious topical treatment. Furthermore, taking into consideration the longer-term effects of phototherapy, it would introduce further complexity to the model because patients continue to use topical treatments in addition to phototherapy. A recent analysis demonstrated that phototherapy reduced, but did not negate, the need for topical treatments over a 1-year period (31). The impact of methotrexate is less clear, as the efficacy may be lower than the topical treatments (32). In addition, we assumed a relapse rate of the topical treatments based on a study that used a different formulation. While this may be the closest available evidence, there is some uncertainty about this estimate. For phototherapy, the relapse rate following 12 weeks of treatment is likely to be lower than 4 weeks of treatment with a topical agent, which again could have an impact on the outcome if the time horizon was extended beyond 12 weeks and the efficacy and potential relapse rates of phototherapy were included. The same may hold true for methotrexate, although the impact is even more uncertain. Further limitations of the model include the assumption that patients without treatment success who received a second 4-week course of topical treatment had a probability of treatment success that was the same as for the initial 4-week treatment period. In clinical practice, non-response to an initial course of treatment may lead to a modification in topical treatment, unless the non-response is due to poor adherence. In addition, the model does not capture the possible long-term side effects (e.g. liver fibrosis) or benefits (e.g. reduced systemic inflammation) of methotrexate, or possible long-term UV damage secondary to UVB (ultraviolet B-rays). Another potential limitation is that local data sources were not used for utility weights in the base-case and sensitivity analyses.
The rising cost of psoriasis treatment presents a challenge (33). Improved topical therapies, such as Cal/BD foam, have demonstrated efficacy in patients with more severe psoriasis (19), and thus have the potential to reduce the need for some patients to progress to phototherapy and/or systemic treatment. In addition, the use of improved topical therapies may lead to lower treatment costs in more severe psoriasis. A recent US budget impact analysis predicted that the introduction of Cal/BD foam has the potential to decrease the annual cost of treatment in patients with moderate-to-severe psoriasis who were previously candidates for treatment with biologics (34).
In conclusion, Cal/BD foam is a cost-effective solution for the treatment of psoriasis vulgaris, dominating over Cal/BD ointment, in this cost-utility analysis conducted from the perspective of a Swedish healthcare payer.
This study was sponsored by LEO Pharma A/S. The authors wish to thank Nanna Julie Nyholm Jensen (BSc Publ Health) for the analysis support. Writing assistance was provided by Andrew Jones (PhD) of Mudskipper Business Limited, funded by LEO Pharma A/S.


 Click to show fullsize
Click to show fullsize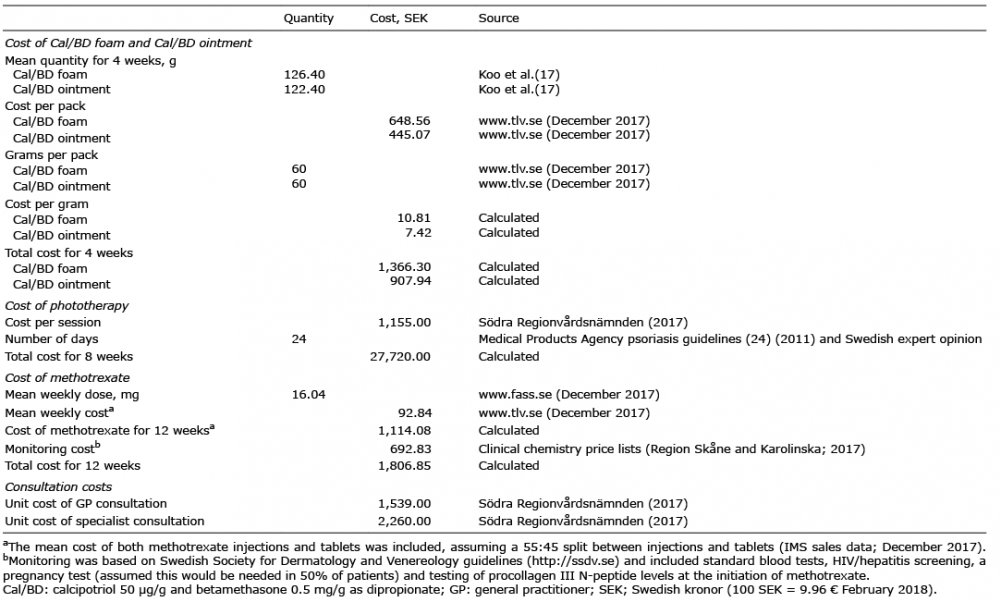 Click to show fullsize
Click to show fullsize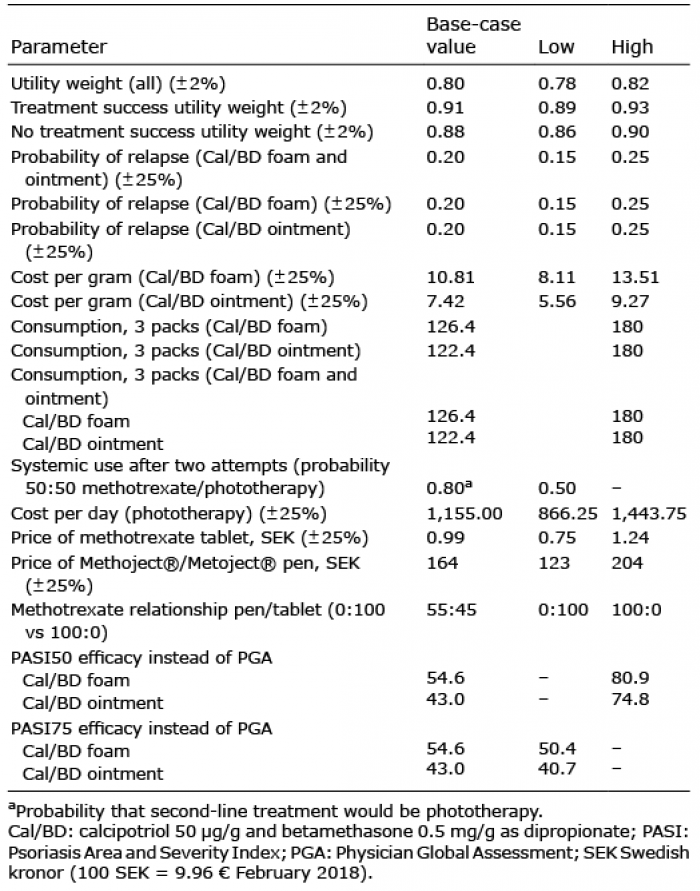 Click to show fullsize
Click to show fullsize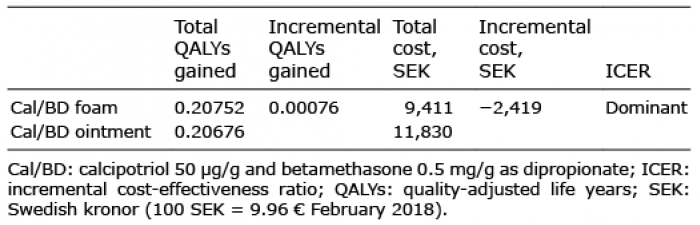 Click to show fullsize
Click to show fullsize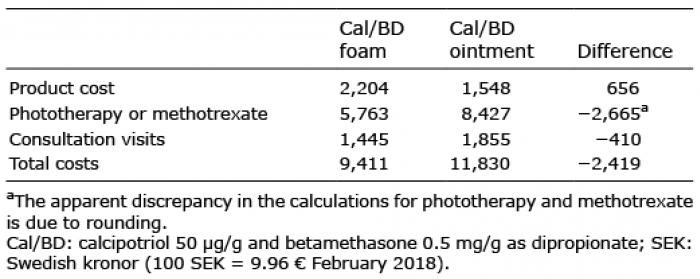 Click to show fullsize
Click to show fullsize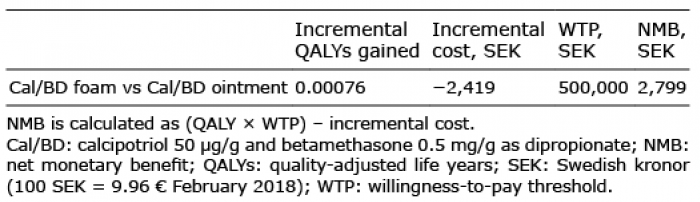 Click to show fullsize
Click to show fullsize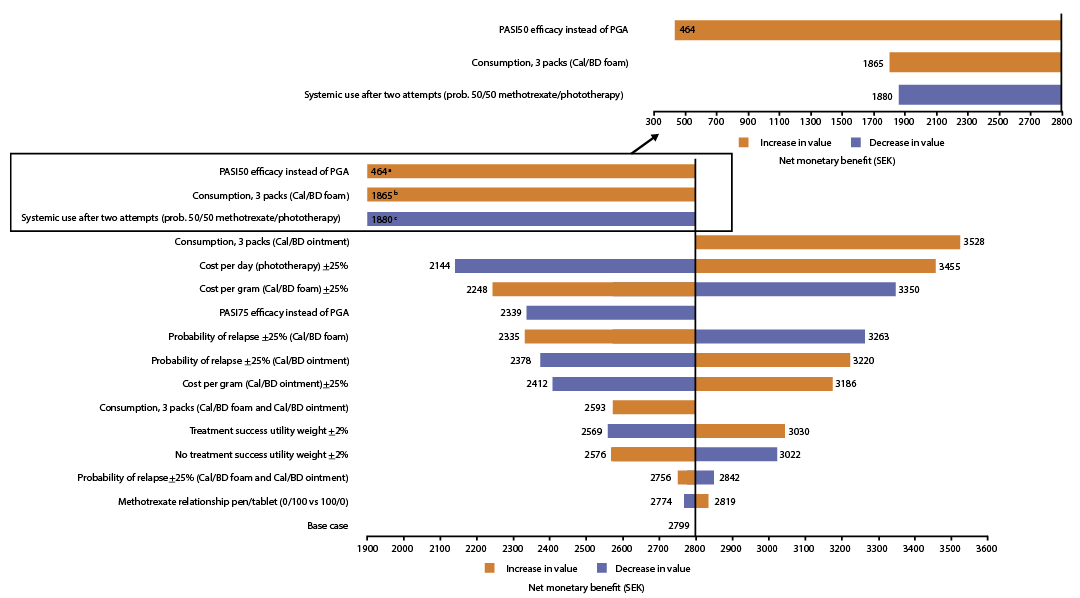 Click to show fullsize
Click to show fullsize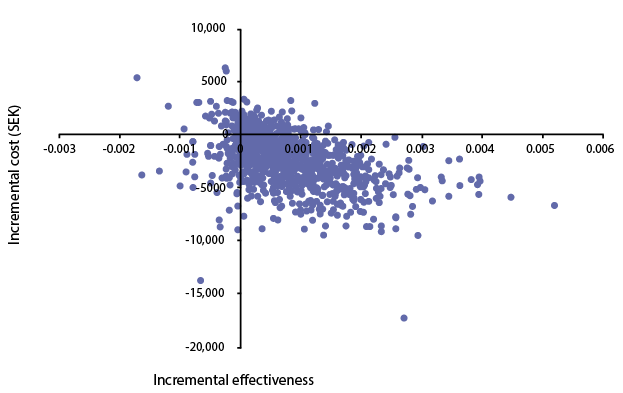 Click to show fullsize
Click to show fullsize