


Departments of 1Dermatology, 3Neurosurgery and 4Radiation Oncology, Hamamatsu University School of Medicine, 1-20-1 Handayama, Higashi-ku, Hamamatsu 431-3192, and 2Radiation Oncology Center, Suzukake Central Hospital, Hamamatsu, Japan. *E-mail: t-shima@hama-med.ac.jp
Accepted Jan 23, 2019; E-published Jan 23, 2019
Balloon cell malignant melanoma (BCMM) is a rare variant of melanoma, first reported by Gardner & Vasquez in 1970 (1). BCMM is histologically characterized by large and polyhedral foamy cells with abundant cytoplasmic vacuoles (2). In general, brain metastasis is common and is a poor prognostic factor in patients with melanoma, even in the era when immune checkpoints and BRAF/MEK inhibitors are used as therapeutic modalities (3). Recent studies have shown that combined stereotactic irradiation (STI) with immune checkpoints or with BRAF/MEK inhibitors can significantly improve overall survival for patients with melanoma brain metastases (4, 5). We report here a rare case of BCMM in which BRAF/MEK inhibitors and subsequent anti-PD-1 antibody (nivolumab) were ineffective, but the brain metastatic lesions were completely resolved by STI in combination with nivolumab.
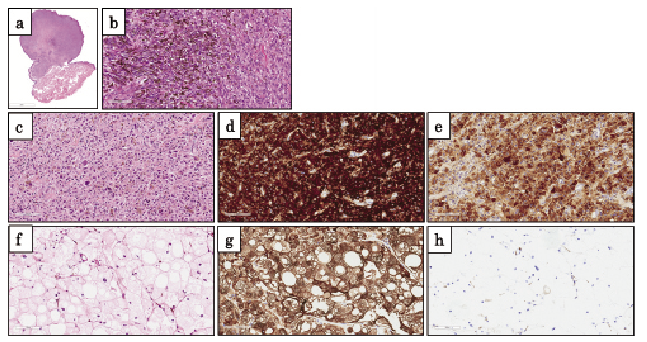
A 71-year-old Japanese woman had a primary nodular melanoma in the right posterior cervix and underwent a wide local excision and sentinel lymph node (SLN) biopsy in the posterior cervix 4 years before she was referred to us. Histopathologically, both the primary lesion (Fig. 1a, b) and SLN showed dense proliferation of large atypical spindle or epithelioid melanocytes. She was diagnosed as having melanoma, stage IIIA (pT4a, N1a, M0; Breslow tumour thickness, 5 mm; Clark’s level IV, without ulceration). She received 3 courses of dacarbazine post-operative adjuvant therapy, followed by monthly interferon-β intralesional injection as maintenance therapy. Two years after the operation, however, she developed multiple metastatic lesions in the lung, abdominal subcutis, and brain without neurological abnormalities. Brain magnetic resonance imaging (MRI) showed an isolated tumour in the right frontal cortex (Fig. S1a). Biopsy specimens obtained from the abdominal subcutaneous nodule confirmed the diagnosis of metastatic melanoma (Fig. 1c), which had the same Melan A+ (Fig. 1d) HMB-45+ (Fig. 1e) cytological phenotype as the primary melanoma, with a BRAFV600E mutation. She was treated with a combination of BRAF (dabrafenib; 300 mg/day) and MEK inhibitors (trametinib; 2 mg/day) with a therapeutic effect on the metastases in the lung and abdominal subcutis, while the size of brain lesion had been unchanged. At 13 months after initiation of BRAF/MEK inhibitors, the metastatic brain lesion expanded from 25 to 41 mm in diameter (Fig. S1b). She underwent a tumour resection, while BRAF/MEK inhibitors continued. Histologically, brain metastatic melanoma showed diffuse proliferation of histiocytoid tumour cells composed of large, polygonal, foamy cells with abundant cytoplasm (Fig. 1f). These tumour cells were positive for Melan A (Fig. 1g), but negative for HMB-45 (Fig. 1h). The resected brain tissue still showed a BRAFV600E mutation. Thus, the melanoma was converted to the balloon cell variant in the metastatic brain lesion. Post-operative brain MRI indicated 3 new brain metastases in the left frontal lobe (Fig. S1c, red circle) and left temporal lobe (Fig. S1d, red circle). Thus, 38 Gy of stereotactic radiotherapy (SRT) for the surgical cavity and 25 Gy of stereotactic radiosurgery (SRS) for brain metastases in the left frontal lobe and left temporal lobe were implemented. Furthermore, the treatment was switched to nivolumab, 3 mg/kg every 2 weeks. However, a new lesion in the left temporal lobe appeared after 3 courses of nivolumab (Fig. S1d, blue circle). To control the brain metastases, SRS (26 Gy) was administered for the new lesion in combination with nivolumab. After a total of 7 courses of nivolumab, all brain metastases disappeared markedly (Fig. S1e, f, arrows). The patient currently maintains a complete response for 9 months after the administration of nivolumab.
Fig. 1. Histopathology of primary lesion, metastases of abdominal and brain lesions. (a and b) Primary melanoma, excisional biopsy. A low-power view of the lesion shows a hemisphere and pedunculated tumour. A high-power view demonstrates large atypical spindle or epithelioid melanocytes. (c) Subcutaneous metastatic melanoma in the abdominal lesion, incisional biopsy. Solid proliferation of polygonal melanocytes with abundant cytoplasm, irregular nuclei, and melanin. (d and e) Immunohistochemical staining of the subcutaneous metastatic tumour, positive for (d) Melan A and (e) HMB-45. (f) Brain metastatic melanoma, excisional biopsy. A high-power view shows histiocytoid, foamy cells with abundant cytoplasm. (g and h) Immunohistochemical staining of the brain metastatic melanoma, positive for (g) Melan A, but negative for (h) HMB-45. Scale bars: (a) 3 mm, (b–h) 100 μm.
Only 4 cases of BCMM with brain metastasis have been reported to date (6–9). In the current case, the cytological balloon cell change was associated with loss of HMB-45 expression. Although BRAFV600E mutation were continuously observed in the rapidly expanded brain metastasis, BRAF/MEK inhibitors were ineffective. Interestingly, a patient developing lymph node metastatic melanoma with balloon change following nivolumab treatment has been documented (10). Thus, BRAF/MEK or immune checkpoint inhibitors may induce the phenotypical changes in melanoma.
As compared with wild-type BRAF, BRAF mutation is an independent predictor of better prognosis in patients with melanoma brain metastases receiving SRS (11). On the other hand, the combination of SRS and immune checkpoint inhibitor (ani-PD-1 antibody or anti-CTLA-4 antibody) is also associated with reduction of distant intracranial failures compared with SRS alone or SRS with BRAF inhibitor (12). X-ray irradiation induces PD-L1 expression in mouse cancer cells, but enhances a tumour-suppressing effect in combination with anti-PD-1 antibody (13). Radiation also allows tumour cells to be more easily recognizable by the immune system, resulting in development of tumour-specific cytotoxic T lymphocytes. Importantly, the administration of immunotherapy within 4 weeks of radiotherapy significantly reduces tumour volume of melanoma brain metastases in comparison with the treatment performed separately for a period longer than 4 weeks (14). Thus, the timing of radiotherapy in relation to immunotherapy and the type of immune checkpoint therapy are issues requiring clarification. It is known that radiotherapy may induce the “abscopal effect”, shrinkage of non-irradiated metastatic tumours distant from the scope of the localized irradiated tumour, suggesting that they may exert synergistic effects (15).
In conclusion, BRAF/MEK inhibitors might have led to balloon cell change in this patient with melanoma. The possibility that new brain metastasis occurring under nivolumab might be a “pseudo-progression” cannot be completely excluded. However, combining anti-PD-1 antibody with radiotherapy effectively reduced tumours and may improve the long-term prognosis of melanoma brain metastases.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize