


1Division of Microbiology, Department of Pathology, Faculty of Medicine, University of Porto and Department of Dermatovenereology, Hospital Centre of S. João, Porto, 2Health Centre of Lapa, Consulta DST, 3Faculty of Medicine, University of Porto (CIDES & CINTESIS), 4National Institute of Health Doutor Ricardo Jorge, Lisbon, and 5Sanofi Pasteur MSD, Portugal
Human papillomavirus (HPV) infection is highly prevalent in the sexually active population. This study estimates the prevalence of HPV DNA in anal and oral samples from a cohort of men and women with incident anogenital warts. Anal and/or oral samples from 541 patients with anogenital warts were tested for 35 HPV genotypes using a PCR assay. The overall prevalence of anal HPV and oral HPV DNA was 59.9% (n = 305/509; 95% confidence interval (CI) 55.6–64.1%) and 14.5% (n = 78/538; 95% CI 11.8–17.7%), respectively. Among patients with perianal warts, the anal HPV DNA prevalence was 92.3% (95% CI 87.0–95.5%). Anal HPV DNA prevalence in patients with genital warts but no perianal warts was 55.7% (95% CI 50.6–60.7%). Both anal and oral HPV infections were more common in men who have sex with men than in heterosexual men (90.4% versus 38.5% and 20.8% versus 11.8%, respectively). Anal high risk-HPV infection was more common in women (58.8%) and in men who have sex with men (67.7%). We found that anogenital warts represent a clinical marker for both anal and oral HPV infections, including anal high risk-HPV infections, particularly among women and men who have sex with men.
Key words: HPV; anal canal; oral mucosa; anogenital warts; epidemiology.
Accepted Feb 5, 2019; E-published Feb 6, 2019
Acta Derm Venereol
Corr: Carmen Lisboa, MD, PhD, Department of Microbiology, Faculty of Medicine. Alameda Prof. Hernani Monteiro, 4200-319 Porto, Portugal. E-mail carlis@med.up.pt
Human papillomavirus infection is highly prevalent in sexually active population and has been associated with anal and oropharyngeal cancers. This study estimates the prevalence of human papillomavirus on anal and oral samples from men and women with external anogenital warts. We found a high prevalence of human papillomavirus on extra-genital sites (anal canal and oral mucosa) among patients with external anogenital warts. Both anal and oral human papillomavirus infections were more common in men who have sex with men than in heterosexual men. Anal high risk HPV types (high risk as carcinogenic) were more common in women and in men who have sex with men. Overall, we demonstrated a high human papillomavirus burden in this population beyond anogenital warts, suggesting a greater impact of human papillomavirus vaccination.
Human papillomavirus (HPV) infection is associated with several different diseases in men and women. Anogenital warts (AGWs) represent the most common sexually transmitted disease (1) and low-risk (LR) HPV genotypes are implicated in these lesions. Nevertheless there is a growing body of evidence that AGWs may be associated with an elevated risk of cancer. Many of these wart lesions shared exposure to the high-risk (HR) HPV genotypes. It has been reported that individuals who had anogenital warts had a higher risk of developing anal and oral cancers (2). Additionally, HPV is highly prevalent in the sexually active population and has been associated with 80–85% of anal cancers (3) and 50% of oropharyngeal cancers (4).
The estimate of oral HPV prevalence reported in two recent systematic reviews was 4.5% (5) and 5.5% (6) in healthy individuals. Furthermore, estimates of anal HPV DNA prevalence ranged from 27 to 43% in women (7, 8), from 12 to 36% among heterosexual men (HM) (9, 10) and from 47.2% to 92.6% among men who have sex with men (MSM), the higher proportions corresponding to HIV-positive MSM (9, 11). Nonetheless, only few studies have evaluated the prevalence of HPV DNA in the anal canal and oral mucosa of patients with AGWs (12). Such data is important to improve our knowledge on the epidemiology of anal and oral HPV infection, namely in patients with AGWs, and ultimately to evaluate the role of prophylactic HPV vaccines in HPV-related diseases of the oropharynx and anal canal.
This study aims to assess the type-specific prevalence of HPV in the anal canal and oral mucosa from patients with AGWs included in the HPV Epidemiological Research on COndyloma LESions (HERCOLES) study (13). Additionally, we evaluated the type-specific HPV DNA concordance among the different anatomical sites analyzed.
The HERCOLES study was a large national, epidemiological and observational study conducted in 7 Investigational Centres, located in mainland Portugal major urban areas. From November 2012 to March 2014 consecutive attendees of the Dermato-venereology and Sexually Transmitted Diseases (STD) Outpatient Clinics with incident clinically diagnosed AGWs were recruited. Additional details of the study design have been described previously (13). Each Centre Ethics Committee approved the study.
Participants were eligible for participation if they were men or women; aged 18–70 years; live in Portugal during the previous year; reported no previous clinical diagnosis of AGWs. All included patients had provided a written informed consent for the participation in the study.
Socio-demographic and sexual behavioural characteristics and some laboratory data of the participants were collected through a Case Report Form. The study included swabbing the AGWs for HPV testing and genotyping. Sampling of the anal canal and oral mucosa were optional and the specimens were collected only if the participant provided additional consent.
AGW samples were collected into individual sterile dry plastic tubes, using saline-wetted Dracon swabs (Digene, USA). Separate specimens were obtained from different locations according the following orientation: location A: pubic region/penile shaft or labia majora; location B: foreskin/corona sulcus/glans/urethral meatus (men) or labia minora/vaginal introitus (women); location C: perineum/groin/scrotum (men); location D: perianal region.
Additional samples from the oral mucosa and the anal canal were collected using a standardised protocol from participants who provided consent. Oral samples were obtained from the tonsillar area using a cytobrush (Biogyn, Italy). Anal samples were collected by inserting a cytobrush (Biogyn, Italy) about 2 cm into the anal canal and rotated 360 degrees.
All samples were stored at –20ºC until they were transported on dry ice to the main Laboratory IPATIMUP Diagnostics. At the main Laboratory the specimens were stored at –70ºC until HPV DNA detection and genotyping were performed.
HPV DNA extraction and HPV genotyping were performed using the CLART HPV2 Test (Genomica, Madrid, Spain), according to the manufacturer instructions. Briefly, this assay is a PCR-based HPV DNA genotyping assay, based on a genotype amplicon-specific hybridization on a microarray. Amplification of a fragment of 450bp into the L1 region, allows the detection of 35 genotypes (HPV 6, 11, 16, 18, 26, 31, 33, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 61, 62, 66, 68, 70, 71, 72, 73, 81, 82, 83, 84, 85, and 89). The assay has two internal controls, a DNA control (human Cystic Fibrosis Transmembrane Conductance Regulator (CTFR) gene) for sample sufficiency, and an amplification control (plasmid) for process control in each reaction.
For statistical purposes, HPV 16, 18, 31, 26, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 70, 73, 82 and 85 were considered as HR-HPV (includes HR and probable HR genotypes) and HPV 6, 11, 40, 42, 43, 44, 54, 61, 62, 71, 72, 81, 83, 84 and 89 as LR-HPV (includes LR and unclassified genotypes) (14, 15).
Only samples that tested positive for any of the 35 genotypes were judged to be adequate and included as positive for HPV in the analysis. Samples in which none of the 35 HPV genotypes were detected were included as HPV negative. Samples were classified as HPV undetermined when the amplification process was inhibited or in the absence of DNA.
Type-specific HPV positivity was expressed as the proportion of HPV-positive cases in which the particular genotype was detected, with or without co-infection by the other genotypes. Multiple HPV was defined as the presence of two or more HR and/or LR HPV genotypes. HPV concordance was defined as detection of the same HPV type in two or more locations in one individual.
Qualitative categorical variables were described as numbers and percentages. Quantitative variables were described using mean and standard deviation or median and interquartile range (IQR), depending on the distribution of the variables. For group comparisons appropriate hypothesis testing was implemented depending on the type of variables compared. Quantitative variables were compared using the t-test, if normal distribution could be assumed, or the nonparametric Mann-Witney U test, if normality could not be assumed. Qualitative variables were studied using the Chi-square test or Fisher’s exact test, as appropriate. All hypothesis tests were two-sided and a p-value less than or equal to 0.05 was considered to be statistically significant. Confidence intervals (95%) around prevalence estimates were determined by the Clopper-Pearson (exact) method.
The study sample size was determined, taking into account the main objectives of the HERCOLES study. Specifically, for the estimation of the prevalence of HPV in the anal canal (n = 509) and oral mucosa (n = 538) we were able to estimate the prevalence proportions with a 95% confidence level and a margin of error of 4.3% and 4.2%, respectively.
Descriptive and inferential analyses were performed using SPSS® v.19.0 (Statistical Package for the Social Sciences).
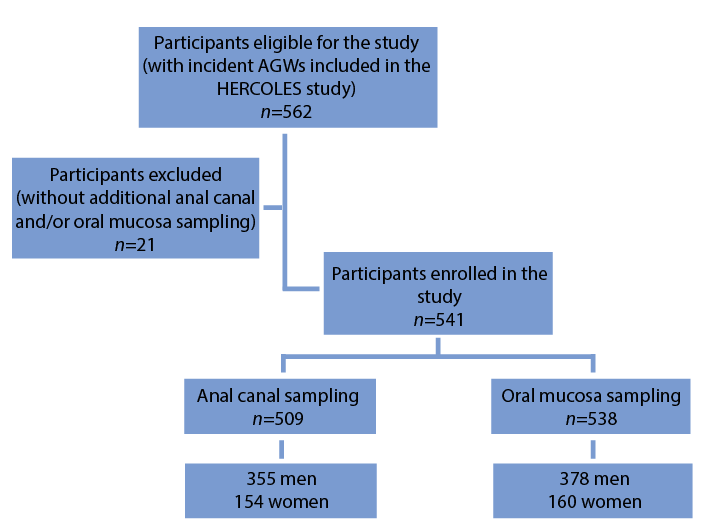
A total of 541 (381 men and 160 women) patients who allowed anal and/or oral mucosa sampling, out of 562 patients with incident AGWs included in the HERCOLES Study, were selected (Fig. 1). Characteristics of these 541 patients are summarized in Table I. The median age of patients was 32 years (18–70 years). The majority of patients were men (381/541; 70.4%) and most of them were uncircumcised (62.5%). Half of the patients were past smokers (50.1%). Most of the participants were heterosexual (86%) and one fifth (74/381; 19.4%) of the men were MSM. A single sexual partner in the year before enrollment was reported by 56.4% of the patients. The proportion of participants who reported having had oral sex and anal intercourse was 71.7% and 47.2%, respectively. Overall, 46% of the patients reported never using condoms with casual partners. At enrollment 10.9% of the patients were HIV-positive, 12.9% had another sexually transmitted infection (STI) and just 2.0% were immunosuppressed, besides HIV infection. Among HIV-positive participants, 47.2% (34/72) were MSM, 5.4% (16/296) were HM and 4.5% (7/155) were women (data not shown).
Fig. 1 Flow chart of participants through the study. AGW: anogenital warts.
Table I. Selected characteristics and sexual behavior of the 541 participants with external anogenital warts
The majority of the AGWs were located on the pubis/penile shaft or labia majora (254/541; 47.0%). Perianal warts were present in 32.7% (177/541) of our study population. They were more common among women (74/160; 46.3%) and MSM (56/74; 75.7%) (data not shown).
Overall, the HPV DNA prevalence in AGWs was 90.2% (95% CI 87.4–92.4%). Anal and oral HPV prevalence was 59.9% (95% CI 55.6–64.1%) and 14.5% (95% CI 11.8–17.7%), respectively (Table II). Anal HPV DNA detection was higher in women than in men (85.1% versus 49%; p < 0.001). Concerning sexual behavior among men, anal HPV DNA detection was more prevalent in MSM than in HM (90.4% versus 38.5%, respectively; p < 0.001) (Table II). We found more undetermined HPV DNA cases in the anal canal of HM (45.2%) than among women (7.1%) or MSM (4.1%) (Table II). Analyzing the group of patients with perianal warts positive for any HPV (n = 161/177), the anal HPV DNA prevalence was 92.3% (95% CI 87.0–95.5%) and no significant differences were found when comparing men and women (Table III). Anal HPV DNA prevalence in patients with genital warts positive for any HPV (with-out perianal warts) (n = 322/364) was 55.7% (95% CI 50.6–60.7%). We found significant differences between men and women (Table IV). Concerning the association between anal HPV DNA detection and anal intercourse among women, we found that 51 out of 131 women, with detectable anal HPV DNA, reported anal intercourse; on the other hand 3 out of 12 women without detectable anal HPV DNA reported this sexual practice (p = 0.54).
Table II. Human papillomavirus (HPV) DNA prevalence in external anogenital warts (n = 541), anal canal (n = 509) and oral mucosa (n = 538) among women, men who have sex with men (MSM) and heterosexual men
Table III. Human papillomavirus (HPV) DNA prevalence in external genital warts, anal canal and oral mucosa among women, men who have sex (MSM) with men and heterosexual men without perianal warts. Both anal and oral prevalence of HPV DNA were estimated among patients with any HPV in genital warts (n = 322)
Table IV. Human papillomavirus (HPV) DNA prevalence in external perianal warts, anal canal and oral mucosa among women, men who have sex with men (MSM) and heterosexual men. Both anal and oral prevalence of HPV DNA were estimated among patients with any HPV in perianal warts (n = 161)
Oral HPV prevalence was higher in MSM than in HM (20.8% versus 11.8%), although the difference was not statistically significant. Among women we found HPV DNA in 16.9% of the oral mucosa samples (Table II).
Multiple HPV types were frequently present in AGWs, anal canal and oral mucosa. Co-infection with multiple HPV types, with at least one HR-HPV, was more common in women (48.9%) and in MSM (55.4%) in the anal canal (Table V). We found a similar prevalence of HR-HPV DNA in AGWs (43.4%), anal canal (51.5%) and oral mucosa (51.3%). In the group of patients with perianal warts the prevalence of HR-HPV DNA in the warts was 48.8% and in the anal canal was 55% (data not shown). In 10.4% of the cases, HPV DNA was simultaneously detected in AGWs, anal canal and oral mucosa.
We found no significant association between HPV DNA detection either in the anal canal or oral mucosa and HIV infection or current medication with immuno-suppressive drugs.
Table V. Distribution of Human papillomavirus (HPV) infection according to low/high risk and single/multiple infections in HPV positive casesa in anal canal, oral mucosa and external anogenital warts among women, men who have sex with men (MSM) and heterosexual men
Type-specific HPV DNA frequency in AGWs, anal canal and oral mucosa is given in Table VI. HPV types with the highest prevalence in AGWs, anal and oral mucosa were HPV 6, 11, 16 and 53. HPV 6 or 11 were the most frequently detected in AGWs (91.6%), anal canal (77.4%) and oral mucosa (65.4%). HPV 16 was present in 9.8% of AGWs, 9.5% of anal canal samples and 7.7% of oral samples. The prevalence of HPV16 in the anal samples, positive for HPV detection, was 10.7% (14/131) among women, 21.5% (14/65) among MSM and 0.9% (1/109) among HM (data not shown). Single infection with HPV 16 was found in the anal samples of 5 patients (2 women and 3 MSM) and in two women’s oral samples. HPV 18 was not detected in any oral samples. HPV type concordance, of at least one genotype, between AGWs and anal canal was found in 83.3% of the cases and between AGWs and oral mucosa in 64.1% of the cases. On the other hand, concordance, of at least one genotype, between perianal warts and anal canal was present in 94.4% of the cases.
Table VI. Type-specific Human papillomavirus (HPV) DNA frequency in external anogenital warts, anal canal and oral mucosa
Few studies have evaluated oral and anal HPV prevalence in patients with AGWs. In this study, a high prevalence of anal HPV infection (59.9%) and oral HPV infection (14.5%) was found among patients with incident AGWs. These data are similar yet slightly higher than those reported by Kofoed et al. (12), who found a prevalence of HPV DNA of 46.2% in the anal canal and of 10.4% in the oral cavity among STI attendees with AGWs. Concerning oral HPV infection, differences in procedures for oral sampling, processing and detecting HPV DNA, in addition to population differences, make it difficult to perform meaningful comparisons between the studies. In our study, oral samples were obtained from the tonsillar area, while Kofoed et al. (12) analyzed oral rinse samples. It is accepted by some authors that oral rinse collection would yield HPV DNA from the entire oral cavity (16). Nevertheless, some studies found a high frequency of HPV in oropharynx, namely in the tonsils (5). The oropharyngeal region seems to be more susceptible to the HPV infection than the oral cavity (5) and a higher prevalence of HPV-related cancer of the head and neck was found in the tonsillar areas (4). We found that oral HPV DNA was more frequently present in MSM (20.8%) than in HM (11.8%). Similarly, reported oral HPV prevalence was considerably higher in MSM without AGWs, with estimates of 12.2% (6) and 13.7% (17). An association between practicing oral sex and oral HPV infection has been reported (6, 18, 19). Yet, other studies stated that oral sexual practices were not associated with oral HPV infection among men or women (16, 20). Presumably, as previously suggested, oro-genital sex and oral to oral contact, such as open mouth kissing, are risky behaviors, associated with oral HPV in a group of individuals, namely young people (18, 21, 22).
We demonstrated a higher prevalence of any HPV type in the anogenital samples than in the oral samples, in accordance with other studies that assessed participants with (12) and without AGWs (17). In this study, men with perianal warts had a higher prevalence of anal HPV DNA than patients without perianal warts. Probably, this reflects the higher number of MSM in this group compared to the group of men with AGWs but no perianal warts. Interestingly, among women the prevalence of anal HPV DNA was not significantly affected by the presence of perianal warts. On the other hand, we found that the detection of any HR-HPV type in the anal samples was markedly more common among women (58.8%) and MSM (67.7%). A systematic review reported that anal HR-HPV prevalence ranged from 23–86% in HIV-negative women with HPV-related pathology of the vulva, vagina and cervix (23). Our finding was included in this range, as HIV-positive women represent only a small proportion of our female cohort. Among the MSM, the reported anal prevalence of HR-HPV was 37.2% in HIV-negative and 73.5% in HIV-positive (11). HPV16 was the third most frequently detected HPV type in the anal samples of our patients with AGWs, and it was particularly prevalent among women (10.7%) and MSM (21.5%). Studies, which analyze the populations without AGWs, found anal HPV 16 prevalence to be around 4% among women (8) and to range 9–27% in MSM (11). In fact, HPV 16 infection and its persistence in the anal canal play an important role in anal cancer development, especially among women and MSM (9, 23).
The present study found a high concordance, of at least one HPV genotype, between AGWs and anal canal/oral mucosa, as reported by other studies (9,12). Some investigators have supported the hypothesis that HPV is transmitted to the oral cavity and anal region via sexual practices. Nevertheless, the role of self-inoculation in spreading HPV infection from AGWs to oral and anal mucosa is unclear; eventually, HPV infection in different anatomical sites should be considered as independent events (9, 24). In our cohort of women with AGWs, sexual practices were not associated with anal HPV infection. In fact, anal intercourse was not a consistent risk factor for anal HPV infection among women (23).
It should be emphasized that a detectable HPV DNA in the oral and anal mucosa of patients’ may not represent a true infection and the virus could be temporarily present for some time.
HPV vaccines have the potential to prevent HPV-related anal diseases (25). Although this evidence remains less robust, concerning the HPV-related oral diseases, the eventual preventive effect of HPV vaccines has been suggested (26, 27). Analyzing our data, the nonavalent vaccine would additionally prevent 1.3% more of AGWs, 4.3% of anal canal infections and 7.7% of oral HPV infection, compared to the quadrivalent vaccine. The potential impact of the nonavalent vaccine would be higher in the anal and oral HPV infections.
This study has some limitations that must be addressed. Firstly, the lower prevalence of anal HPV in HM may reflect the high number of undetermined HPV in the anal samples from HM. This lesser quality of anal canal specimens in HM was previously reported by Nyitrav et al. (9). They postulated that receptive anal sex practices allowed a better collection of exfoliated cells from MSM. In fact, it seems that the presence of unknown inhibitors in the anal canal specimens is lower among both MSM and women. The proportion of undetermined HPV in both women and MSM, found in our study, was in agreement with other studies (9, 28). Secondly, the possible inclusion of participants with unobserved intra-anal/rectal warts may affect the finding of LR-HPV. It is possible that our estimates on anal HPV prevalence also included some HPV present in the perianal region; in the same way as perianal warts could harbour anal HPV. Proctologic examination was not performed in these patients. In our study perianal warts were cutaneous warts located in the perianal area without visible warts at the anal verge. Concerning oral sex, the analysis was limited, as active/passive sex was not ascertained. Nevertheless, we analyzed the association of HPV DNA in the anal canal and anal intercourse, among women. Among men, the analysis was based on sexual behaviors, reflecting differences in sexual practices. The small number of HIV-positive and immunocompromised participants limited the analysis of this group of patients. Lastly, the study population was selected from the attendees of Dermato-venereology and STD Outpatient Clinics and may, in a way, limit the generalizability of the estimates presented.
In conclusion, we found a high prevalence of HPV DNA in the anal and oral samples from men and women with external AGWs. AGWs seem to represent a clinical marker for both anal and oral HPV infections, including anal HR-HPV infections, particularly among women and MSM. We demonstrated a high HPV burden in this population, beyond AGWs, suggesting a greater impact of HPV vaccination. More evidence is needed concerning the natural history of both anal and oral HPV infections and research advancements in order to achieve the best scree-ning strategies for anal and oral HPV-related diseases.
The authors would like to thank the following for their valuable contributions to this study: Joana Cavaco Silva, Patrícia Sousa, Renato Bastos, and Tania Caseiro (KeyPoint). The authors are grateful to the patients who joined the study.
HERCOLES Study Group members and co-authors: Centro de Saúde da Lapa: J.Azevedo, I. Santo; M. Marcelino; Centro Hospitalar Universidade de Coimbra: J.P. Reis, A.R. Portelinha, A.R. Cabral, M.I. Coutinho, M. Gouveia, V. Barreto Teixeira; Hospital Braga: C. Brito, J.C. Fernandes, C. Araújo, C. Resende, O. Ferreira; Hospital Curry Cabral: J. Cardoso, C. Fernandes, A. Rodrigues, A. Laureano, P. Vale Fernandes, T. Mestre; Hospital Garcia de Orta: E. Bártolo, D. Matos, H. Barreiros, J. Alves, R. Coelho; Universitário do S.João: C. Lisboa, C. Moreira; Hospital de Santa Maria: J. Borges-Costa, A. I. Gouveia, A. Teixeira, L. Lopes, L. Uva; Faculdade de Medicina da Universidade do Porto (CIDES & CINTESIS): L. Azevedo, C. Dias C; IPATIMUP Diagnostics: J.C. Machado, L. Cirnes, A. Faustino; SPMSD Portugal: M.J. Cunha, S. Santos.
This study was sponsored by Sanofi Pasteur MSD, Portugal.
Conflicts of interest. MJC was a SPMSD Portugal employee. The other authors declare no conflicts of interest. AP, CL, IS, JA, and LA received occasional grants to attending scientific meetings from SPMSD Portugal.


 Click to show fullsize
Click to show fullsize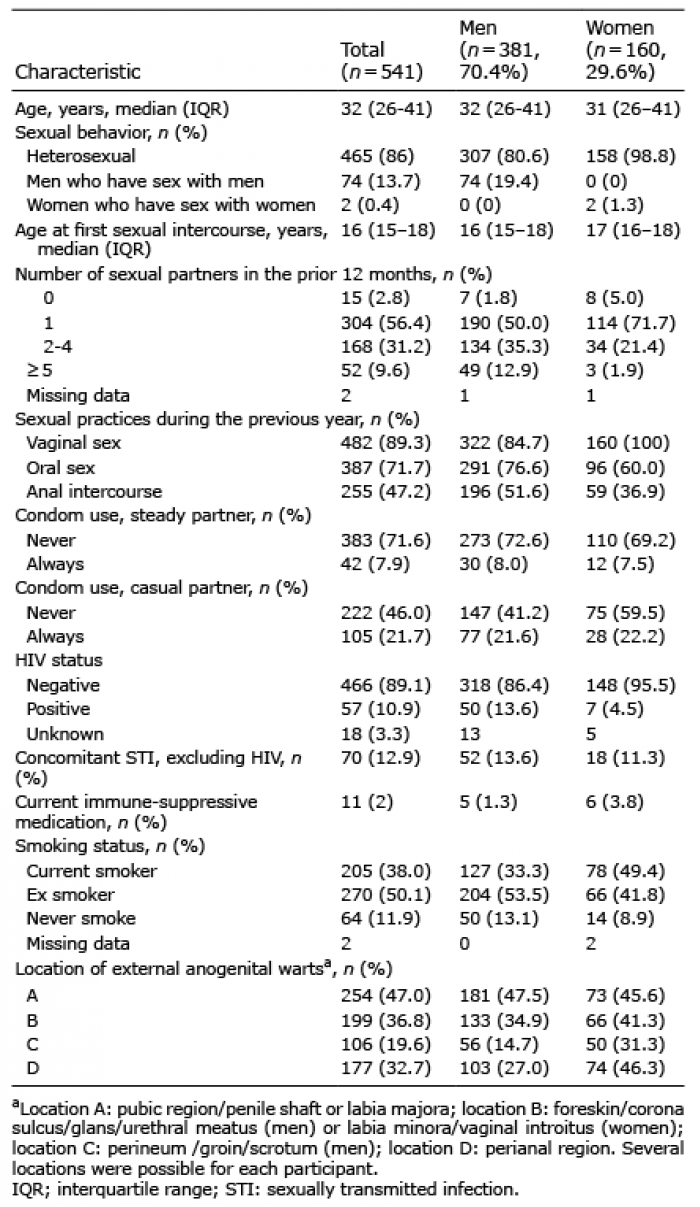 Click to show fullsize
Click to show fullsize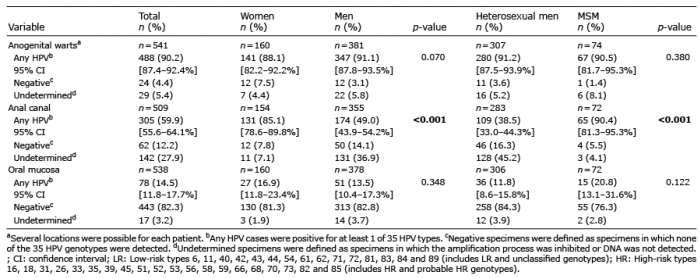 Click to show fullsize
Click to show fullsize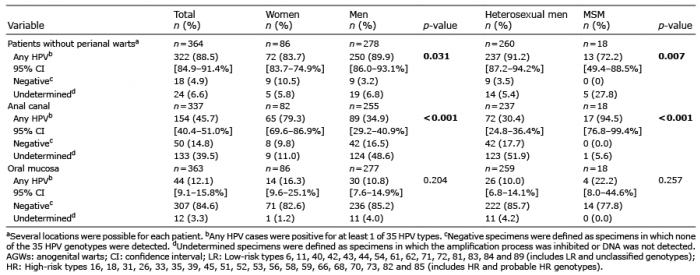 Click to show fullsize
Click to show fullsize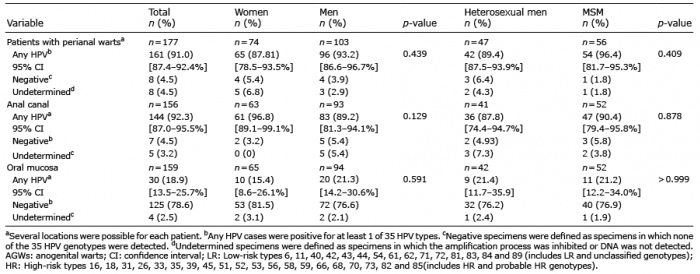 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize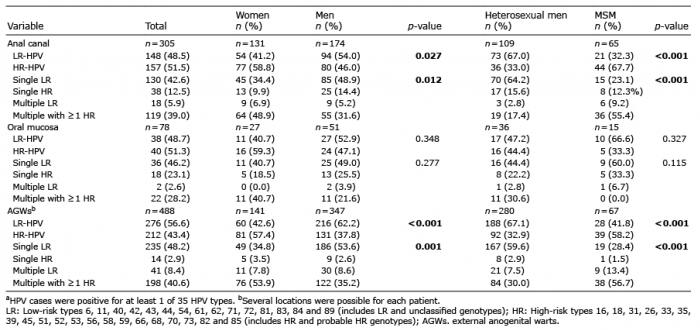 Click to show fullsize
Click to show fullsize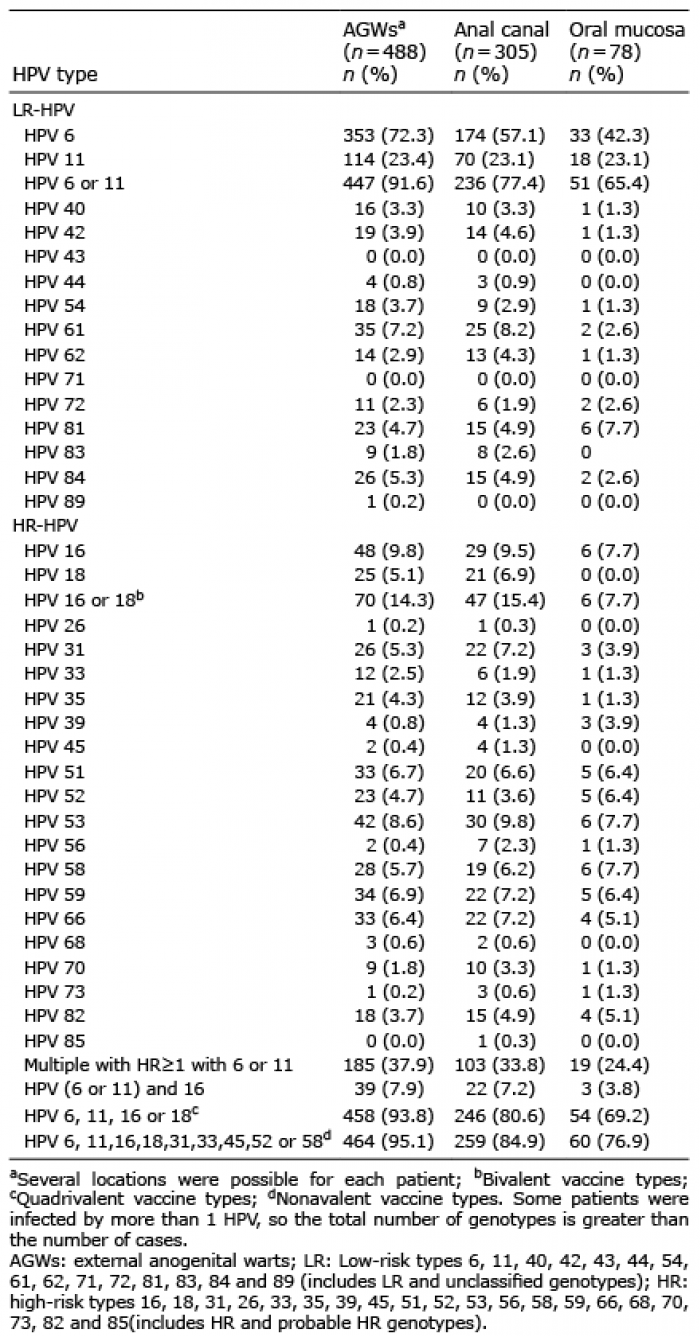 Click to show fullsize
Click to show fullsize