


1Faculty of Health Sciences, University of Southern Denmark, 2Department of Dermatology and Allergy Centre, Odense University Hospital, and 3Odense Patient data Explorative Network OPEN, University of Southern Denmark, Odense, Denmark
The incidence of non-melanoma skin cancer and malignant melanoma is increasing. Diagnosing these skin lesions is primarily done visually, making it suitable to use new technology, such as teledermoscopy. Before the implementation of teledermoscopy, patient satisfaction, clinician satisfaction and diagnostic accuracy, need to be evaluated. A cross-sectional quantitative survey was conducted to evaluate patient satisfaction and expectations regarding a mobile teledermoscopy service, and to identify factors influencing patient satisfaction and choice of diagnostic method. A total of 287 out of 476 participants responded to the questionnaire. Almost 90% of respondents were satisfied with, or neutral towards, teledermoscopy. No associations between patient satisfaction and age, smartphone/tablet usage, travel time, prior history of non-melanoma skin cancer and malignant melanoma, or worries about malignancy, were found. There was equal distribution between patients who preferred tele-dermoscopy and those who preferred face-to-face consultation. Respondents with a high level of smartphone usage significantly preferred teledermoscopy.
Key words: telemedicine; patient satisfaction; skin cancer; malignant melanoma.
Accepted Mar 12, 2010; Epub ahead of print Mar 17, 2020
Acta Derm Venereol 2020; 100: adv000117.
Corr: Sofie Gilling, Faculty of Health Sciences, University of Southern Denmark, Kløvervænget 22B, 11, DK-5000 Odense C, Denmark. E-mail: sofie.gilling@outlook.com
Mobile teledermoscopy enables enlarged photographs of suspicious skin changes to be taken in general practice and sent for evaluation by a specialist. Patient satisfaction and expectations regarding this new diagnostic method need to be evaluated before implementation. The aim of this cross-sectional study was to evaluate patient satisfaction and expectations regarding mobile teledermoscopy, and to identify factors influencing patient satisfaction and choice of diagnostic method. A total of 287 out of 476 participants responded to the questionnaire. Almost 90% of respondents in this study were satisfied with, or neutral towards, mobile teledermoscopy. Respondents equally preferred mobile teledermoscopy or seeing the dermatologist face-to-face, but mobile teledermoscopy was preferred among respondents with a high level of smartphone usage. There is an increasing incidence of skin cancer and melanoma, which calls for alternative ways to diagnose these diseases. Patient satisfaction with teledermoscopy will make implementation more successful.
The incidence of non-melanoma skin cancer (NMSC) and malignant melanoma (MM) is increasing, and they are among the 6 most common types of cancers, in Denmark. In 2017 the total number of people in Denmark diagnosed with NMSC and MM was 16,006 and 2,504, respectively, which has a population of 5.8 million (1, 2). From 1985 through 2012 there was an estimated yearly increase in the incidence of MM in Denmark, by 4.5% for men and 4.3% for women (3). MM occurs in all ages and its frequency increases with age (4). For NMSC, the estimated yearly increase from 2012 to 2016 was 0.5% for men and 0.7% for women (5). Furthermore, the waiting time to see a dermatologist may be weeks to months. This calls for alternative ways to triage and diagnose NMSC and MM, and lower the number of unnecessary referrals.
Suspicious skin lesions are primarily diagnosed visually, thus the use of teledermatology (TD) is suitable.
TD can be classified as “live interactive” or “store-and-forward”. Live interactive TD is synchronous and uses video-conferencing, permitting immediate interaction with the patient. Store-and-forward TD uses photographs for communication, and allows for asynchronous evaluation of the photographs, but lacks immediate interaction with the patient (6–8). One of the newer modalities of store-and-forward TD is mobile teledermoscopy (mobile TDS). A dermatoscope is attached to a smartphone, to convert it to a digital dermatoscope which can store and send photographs. The photographs can be taken in general practice, or elsewhere, and sent directly to a specialist for evaluation.
Diagnostic accuracy and the satisfaction of clinicians and patients need to be evaluated before implementation of mobile TDS. A high level of patient satisfaction and awareness of patient expectations of a mobile TDS service is likely to make implementation more successful.
There are no formally validated questionnaires of patient satisfaction with mobile TDS and TD. Questionnaires used in previous studies that are validated to some extent are face validated or adapted from validated questionnaires (9–12). Face validity is a subjective validity assessment, and means that the questionnaire contains reasonable and relevant common-sense questions (10). The majority of previous studies on patient satisfaction with TD include several skin diseases, e.g. psoriasis, MM, NMSC, eczema and nail disorders, and only a few studies are of a single skin disease, e.g. leg ulcers, acne vulgaris, psoriasis or MM (11, 13–17).
It was hypothesized that patient age, travel time to the skin cancer clinic, prior history of, and worries about having, skin cancer, and familiarity with the use of smartphones/tablets could influence patient satisfaction and attitudes towards mobile TDS.
The objective of this study was to evaluate patient satisfaction with, and expectations of, mobile TDS for diagnosing NMSC and MM in general practice. Secondly, to identify factors influencing patient satisfaction and the patient choice of diagnostic method.
This cross-sectional survey was conducted in the Region of Southern Denmark in January and February 2019 on patients participating in the study “Evaluation and implementation of teledermoscopy in general practice”. The Danish Data Protection Agency approved the study (no. 18/40373). Approval from the ethics committee was not necessary according to Danish legislation.
“Evaluation and implementation of teledermoscopy in general practice”
This study was conducted from January to October 2018. The aims of the study were to compare the diagnosis of suspicious skin lesions achieved by mobile TDS in general practice with traditional face-to-face (FTF) consultations with a dermatologist, and to calculate the change in mean costs per patient through implementing mobile TDS. General practitioners from 48 general practices in the Region of Southern Denmark recruited patients over the age of 18 years, who had skin lesions suspicious of cancer, which the general practitioner wished to refer for a dermatological evaluation. Informed consent was obtained from all patients before inclusion. In addition, patients were asked to give consent to participate in a survey on patient satisfaction. TDS photographs of the skin lesions were obtained by the clinic staff at the general practice with an iPhone® (Apple Inc., Cupertino, USA) and a Handyscope® (FotoFinder Systems GMbH, Bad Birnbach, Germany). The photographs were sent securely via FotoFinder Hub® (FotoFinder Systems GmbH) to the Department of Dermatology and Allergy Centre at Odense University Hospital for evaluation. As part of standard procedure, the patients were also referred to the skin cancer clinic at the Department of Dermatology and Allergy Centre, Odense University Hospital. One of 4 consultant dermatologists had a FTF consultation with the participant, which included a total-body skin examination. Two other consultants from the group reviewed the TDS photographs independently, classified the lesion as benign or malignant, and suggested a diagnosis and treatment plan. The results will be reported elsewhere.
Questionnaire
No formally validated questionnaires exist for patient satisfaction with TD, therefore, questions from previous studies and new questions relevant to the current study were used (9, 11, 12, 18, 19). A quantitative questionnaire was designed to be able to gather a large amount of information from many participants, test our hypothesis and compare data with previous studies. The questions from previous studies were translated from English to Danish without back-translation and validation, as the questions themselves were not formally validated. The questionnaire was adaptive, hence the content and number of questions depended on the answers given by the participants. The number of questions ranged from 34 to 67 in a completed questionnaire. The questionnaire contained multiple-choice questions, Likert scale questions, dichotomous questions, and an option to comment in free writing at the end of the questionnaire. A Likert scale is a 5-point scale, where the participant can express their level of agreement or disagreement, or a neutral attitude with a statement.
Data were collected on demographics, the consultation at the general practitioner and the skin cancer clinic, IT skills, patient satisfaction, expectations towards a mobile TDS service, and data for a socioeconomic analysis. The socioeconomic analysis will be reported elsewhere.
The questionnaire was pilot-tested in 5 of the recruited participants, and they were subsequently interviewed to ensure understanding and relevance of the questions. These 5 participants were excluded from the survey. Thereafter, the face validity of the questionnaire was peer-reviewed by 3 consultant dermatologists.
Squamous cell carcinoma and basal cell carcinoma were defined as NMSC.
Data collection and data management
The participants were sent an invitation to their secure digital mailbox with a link to the questionnaire 2–12 months after their consultation at the skin cancer clinic. The questionnaires were completed online by the participants, and data were submitted directly to a database. Participants having difficulties with their secure digital mailbox were offered the questionnaire in paper form by post. Data from questionnaires in paper form were entered manually to the database and double-checked. If the patients had not completed the questionnaire within 2 weeks the invitation and link to the questionnaire were sent to the secure digital mailbox again. Study data were collected and managed using REDCap (Research Electronic Data Capture) hosted at OPEN (Open Patient data Explorative Network) Odense University hospital (20, 21).
Variables
Patient satisfaction was defined from 10 questions and each question resulted in a score of 1–5 depending on the answer (Appendix SI). The total score was divided by 10 (the number of questions). The satisfaction scale included 5 levels, ranging from very satisfied to very dissatisfied (Appendix SI).
Multiple-choice answers were categorized into 2 groups for the χ2 test. The satisfaction levels were combined into a not-satisfied group, consisting of “neither”, “dissatisfied” and “very dissatisfied”, and a satisfied group, consisting of “satisfied” and “very satisfied”. The age was categorized into < 65 years and ≥ 65 years, and travel time to the skin cancer clinic into < 1 h and > 1 h. For the questions on how often the participants use their smartphone/tablet (phone calls not included), the answer “Many times a day/10 times a day” was defined as a high level of smartphone/tablet usage and the answers “A couple of times a day”, “A couple of times a week or less” and “No usage” were defined as a low level of smartphone/tablet usage. Worries about having NMSC/MM were categorized into not worried and worried, and the “neither” group was excluded from the analysis.
Statistical analysis
Descriptive statistics were used to analyse data, and data are given as proportions. χ2 test was used to test the significance of associations between the groups for categorical variables. Statistical significance was defined as p < 0.05. Data were analysed using STATA (version 15.0).
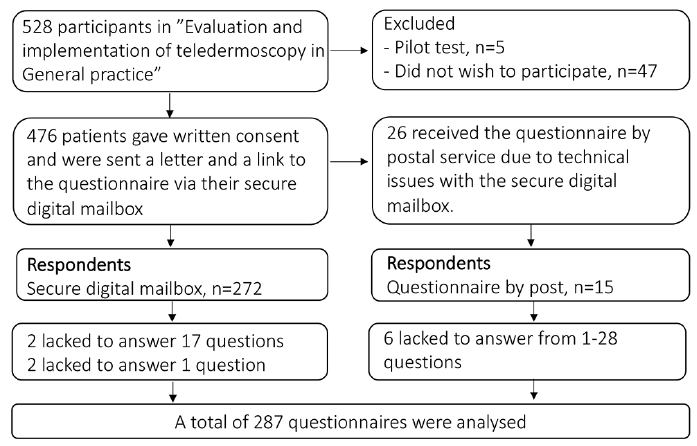
Of the 476 patients consented to receive the questionnaire, 287 (60.3%) responded to the questionnaire. Participants who only responded to the demographic questions were categorized as non-respondents (n = 8). Ten of the respondents omitted to answer between 1 and 28 questions (Fig. 1). More females than males responded to the questionnaire (59.9% female). There was no significant difference between respondents and non-respondents regarding sex.
Fig. 1. Study population flow chart.
Participants younger than 30 years were less likely to respond to the survey (response rate 33.3%) whereas participants aged 60–69 and 70–79 years had response rates of 70.6% and 74.7%, respectively. The median age of the respondents was 60 years (range 20–92 years), and of the non-respondents 52 years (range 19–94 years), both groups being older than the general Danish population, which has a median age of 50 years for people between 19 and 94 years. The median age of the general Danish population was calculated based on data from Statistics Denmark (22).
More respondents were married, fewer were divorced, and their educational level was higher compared with the general Danish population (22, 23).
Approximately 14.0% of respondents reported a previous history of NMSC (n = 33), MM (n = 9), or both (n = 2). A total of 25.4% reported being diagnosed with either NMSC (n = 40) or MM (n = 24) in the study; 9 respondents did not know if they were diagnosed with NMSC or MM.
Of the respondents, 34.1% (89/261) were more than 1 h travel time from the skin cancer clinic. The majority of respondents (74.0%) were seen at the skin cancer clinic within 8–28 days, 16.8% were seen within 7 days, and 9.2% were seen after more than 28 days from the time of the referral.
Patient satisfaction and choice of diagnostic method
More than half of the patients were satisfied and only a few were dissatisfied. To the question “Which diagnostic method would you prefer if teledermoscopy and face-to-face consultation by the dermatologist are equivalent in ensuring a correct diagnosis?” 51.4% of respondents answered “Teledermoscopy at my general practitioner” and 48.6% of respondents answered “Face-to-face consultation at the dermatologist”. Most respondents (80.9%) wanted mobile TDS available as an alternative to a FTF consultation. Overall, 74.8% of respondents preferred to discuss their skin change with the dermatologist at the hospital and 58.1% would feel that something important was missing if they did not see the dermatologist in person. The greatest concern, if the participant only had TDS photographs taken, was that the diagnosis based on TDS photographs would differ from the diagnosis at a FTF consultation.
No significant association was found when comparing the patient satisfaction groups (satisfied and not satisfied) with the variables regarding age, travel time to the skin cancer clinic, history of NMSC or MM, worries of having NMSC/MM, or smartphone/tablet usage.
When comparing the variables regarding age, travel time to the skin cancer clinic, history of NMSC or MM, worries of having NMSC/MM, or smartphone/tablet usage to the preferred diagnostic method, the respondents were more likely to choose TDS if they had a high level of smartphone/tablet usage (p = 0.037), and respondents who were not worried about having NMSC or MM preferred FTF consultations (p = 0.022). Not surprisingly, respondents who were satisfied would rather choose TDS and respondents who were not satisfied would rather choose FTF consultation (p < 0.001).
Expectations
The majority of respondents (71.8%) would use mobile TDS if it meant they would get a more rapid response to whether their skin change is benign. Approximately half of the respondents (48.9%) were willing to wait 5–10 days or more to get the results of the TDS.
Acceptance of being photographed was high (> 95%) regarding the face, upper body (excluding the breasts for females), arms and legs. Only 70.4% accepted having their genitals photographed for TDS. Acceptance among females of having their breasts photographed was lower than for other areas of the body (92.4%), except for the genitals. Two men were not willing to be photographed at all.
To our knowledge, this is the largest study on patient satisfaction with mobile TDS for diagnosing NMSC and MM in general practice. Almost 90% of participants were satisfied or neutral towards mobile TDS. We did not find any factors that were significantly associated with patient satisfaction. There was equal distribution of respondents who preferred TDS and FTF consultations, but respondents with a high level of smartphone/tablet usage preferred mobile TDS as a diagnostic method.
Patient satisfaction and choice of diagnostic method
A recent systematic review of patient satisfaction with TD concluded that the level of satisfaction with store-and-forward TD was high (24). The studies in the systematic review have different definitions of patient satisfaction, and some studies do not define patient satisfaction, making the comparison of studies difficult. In the studies that quantified patient satisfaction as a percentage, the group of satisfied participants ranged from 77% to almost 100%, except for one study, in which only 42% of participants were satisfied (25–33). Our results are in line with the review, although the level of satisfaction is lower compared with the previous studies. The majority of studies in the systematic review included a variety of dermatological diseases, from benign to malignant, which could have had an influence on patient satisfaction. Another reason for the lower level of patient satisfaction in our study could be our definition of patient satisfaction. The items in the satisfaction scale do not differ in the level of importance, and some items will probably affect the level of satisfaction more than others (Tables I and II).
Table I. Patient satisfaction
Table II. Preferred diagnostic method
The severity or consequence of the suspected disease might influence the patients’ perceptions of mobile TDS and affect the importance of talking to the consultant dermatologist. Mofid et al. (34) found that patients being seen for skin cancer or moles were more reluctant to use telemedicine. Qualitative data from another study suggested that the seriousness of the problem was the main factor influencing the preference (9). These previous findings could explain the results in our study, in which only approximately half of the participants preferred mobile TDS. In studies enrolling a variety of dermatological diseases, the preference of TD over FTF consultations was higher than in our study (12, 26). The current study found that the majority of respondents (74%) preferred to talk with the consultant dermatologist about their skin lesion, but in a study enrolling a variety of dermatological diseases only 38% preferred to talk with the consultant dermatologist about their skin disease (25). A concern patients had with store-and-forward TD was a lack of interaction with the consultant dermatologist, and in one study this concern was especially prevalent among elderly subjects (31, 35). The respondents in our study were more concerned about diagnostic accuracy.
A study from Israel found that patients living in rural areas had a significantly higher level of satisfaction than patients in urban areas (28). Our study did not find that participants living further away from the skin cancer clinic had a higher level of satisfaction or a different preference of diagnostic method. This could be due to distances in Denmark not being large enough to have an influence, or that our study population was socioeconomically and culturally different.
Contrary to expectations, the current study found a significant association between respondents who were not worried about having NMSC or MM and the preference of FTF consultation. The explanation of this result could be due to recall bias, the respondents not looking for a quick clarification of whether their skin lesion was benign or malignant, or that they had other dermatological problems they wished to discuss with the consultant dermatologist.
Participants using their smartphone/tablet many times a day preferred mobile TDS. This result was not surprising, as it was expected that participants who had integrated technology into their lives would be more positive towards new technology.
Expectations
Waiting time appears to play an important role in preferring TD over FTF consultation. In our study 71.8% respondents preferred mobile TDS if they got a quicker answer as to whether their skin lesion was benign or malignant. In the study by Collins et al. (9), 76% agreed that they would rather have their skin problem managed via telemedicine than have to wait a few weeks to see the consultant dermatologist in person. The qualitative findings of Collins et al. highlight the importance of short waiting time for an appointment and treatment (9). This is highly relevant in the current Danish setting, where waiting times can be weeks to months. We expect to reduce the waiting time from referral to diagnosis by implementation of mobile TDS. In a Swedish study TDS photographs could be assessed within 24 h (36).
The procedure of mobile TDS, in which several photographs (overview, close-up and dermoscopic) are taken, could be uncomfortable for some patients, especially considering intimate body parts. In the current study the acceptance of being photographed was high, except for the genital area, where only 70.4% wanted to be photographed. Similar to our study, a study from Spain exploring medical photography found that only 70.2% would consent to photography in the case of genital lesions (37). A study from Botswana found that 92% of participants were willing to have their genitals photographed, but only 58% were willing to have their face photographed (12). These findings indicate that there are cultural differences, which are important to consider in the implementation of mobile TDS.
Questionnaire
There was no validated questionnaire or patient satisfaction scale suitable for this study. Although the patient satisfaction scale and the choice of diagnostic method are linked, the fact that satisfied respondents preferred mobile TDS and not satisfied respondents preferred FTF consultation indicates that the scale, to some extent, is acceptable. The level of patient satisfaction in this study is inconsistent with how many prefer mobile TDS (51.4%) and how many would like mobile TDS as an alternative to FTF consultation (80.9%). Previous studies have found similar results where there is high patient satisfaction, but fewer who prefer TD over FTF consultations (9, 10, 32, 38). The fact that the majority of respondents would like mobile TDS as an alternative could indicate that mobile TDS is acceptable and a good solution if FTF consultations are not available. The satisfaction scale is unlikely to identify whether the implementation will be successful, but it may indicate whether patients will receive the new diagnostic method positively. The individual questions in the questionnaire may indicate which areas it is important to focus on in future studies or when implementing the service.
Strengths and limitations
This study has some limitations. First, at the start of the study “Evaluation and implementation of TDS in general practice” the patient satisfaction questionnaire was not ready. This resulted in an inexpedient gap of up to 12 months from the time of FTF consultation at the skin cancer clinic to receiving the questionnaire, possibly leading to recall bias. Recall bias will most likely affect the questions concerning worries about malignancy and the perception of the mobile TDS procedure. Some of the questions are hypothetical, and therefore not as likely to be subjected to recall bias.
Secondly, self-selection bias is a limitation. The participant first had to agree to participate in the study at their general practitioner. This could result in a longer travel time, as they had to be seen at a FTF consultation at the skin cancer clinic instead of a nearby private consultant dermatologist. In addition, the participants had to respond to the survey. The respondents may generally be more interested in new technology, have the resources to travel further for their FTF consultation, and be able to complete an online questionnaire. The study population had more resources, in terms of a higher educational level, and more were married, compared with the general population. Our study population might therefore not be representative of the patients with suspicious skin lesions being referred for a dermatological evaluation.
Participants’ skin lesions were evaluated by both mobile TDS and FTF consultations. Unlike an implemented mobile TDS service, the participants did not lack interaction with the consultant dermatologist and, furthermore, did not have to rely on the TDS diagnosis.
Finally, the current study is limited by the response rate and not knowing the demographic data on the non-respondents.
The strengths of the study include the large number of participants compared with previous studies. In addition, only patients with skin lesions that were suspected to be malignant were enrolled in the study. As discussed previously, the severity of the dermatological disease can influence the perception of mobile TDS. The fact that the questionnaire was electronic made it more convenient for participants to respond, but may have excluded participants with limited IT skills.
Perspectives
The implementation of mobile TDS could be beneficial for patients, especially socioeconomically disadvantaged patients. A study by Ibfelt et al. (39) found that male sex, older age, shorter education, lower income, living without a partner, and residence in specific rural regions of Denmark increased the risk of advanced-staged melanoma at the time of diagnosis. In addition, one of the regions with a higher number of advanced-staged melanoma had only half as many treatment centres for dermatology/plastic surgery as the Capital Region (39). In a pilot-study by Kips et al. (38) patients expressed that TD would encourage them to consult a general practitioner sooner when experiencing dermatological problems. A nearby diagnostic solution will make it more convenient for the patient, especially the disadvantaged patient, which could encourage them to seek dermatological help earlier. Furthermore, as many as 40% of patients referred for NMSC or MM could be managed without a FTF consultation, and the waiting time until diagnosis would also be reduced (36). A major reduction in referrals could free up time for treatments.
Conclusion
In this study, mobile TDS is acceptable to the majority of the respondents referred with skin lesions of concern (NMSC and MM). No associations were found between patient satisfaction and age, level of smartphone/tablet usage, travel time to the skin cancer clinic, prior history of NMSC and MM, or worries about malignancy. A high level of smartphone/tablet usage was associated with preferring mobile TDS. The waiting time from referral until diagnosis, and the dermatological disease appear to influence the preference for mobile TDS. Not seeing a consultant dermatologist at the hospital is a concern for the majority of respondents. The technology is constantly evolving, and therefore evaluations of patient satisfaction will regularly need to be updated. Future studies on patient satisfaction with TD would benefit from a validated patient satisfaction questionnaire and separating malignant and benign dermatological diseases when evaluating the service.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize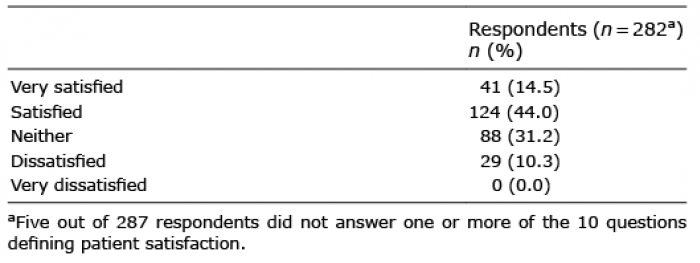 Click to show fullsize
Click to show fullsize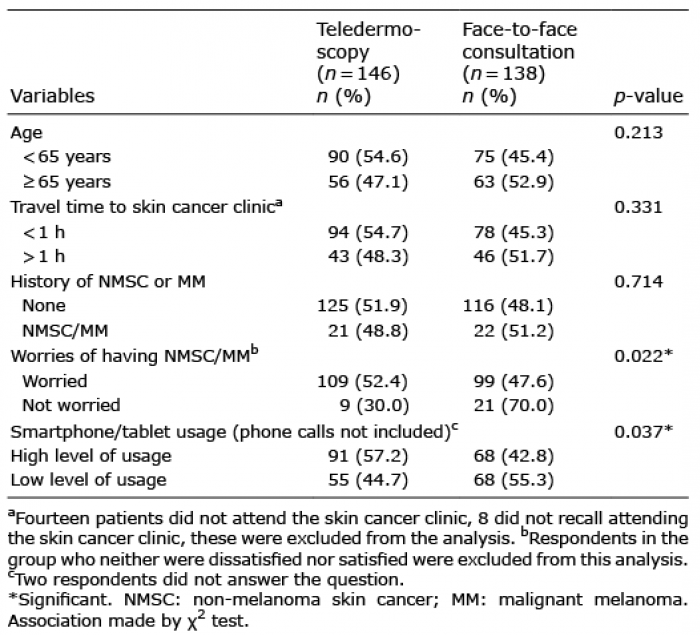 Click to show fullsize
Click to show fullsize