


1Division of Dermatological Allergology, Department of Dermatology, 2Department of Dermatology and 4Department of Pathology, Faculty of Medicine, and 3Gyula Petrányi Doctoral School of Allergy and Clinical Immunology, University of Debrecen, 98. Nagyerdei krt., HU-4032 Debrecen, Hungary. *E-mail: anikokapitany@gmail.com
#These authors contributed equally to this work and should be considered as first authors. §These authors contributed equally to this work.
Accepted Jun 1, 2020; Epub ahead of print Jun 9, 2020
Acta Derm Venereol 2020; 100: adv00203
Recent studies have found different microbiota and chemical milieus in different healthy skin areas. In addition, topographically distinct immune and barrier characteristics have been identified (1–3). Based on these results, the skin cannot be considered a unified organ: 3 different skin niches can be distinguished: sebaceous gland poor (SGP), sebaceous gland rich (SGR), and apocrine gland rich (AGR) skin regions (1, 3). Certain immune-mediated skin diseases localize primarily to one of these regions; for example, atopic dermatitis appears mostly in SGP regions, acne and rosacea appear in SGR regions, and hidradenitis suppurativa in AGR regions.
Other skin diseases can develop in any skin regions, like psoriasis, where lesions can manifest in either SGP regions (psoriasis vulgaris of SGP skin), or SGR regions (scalp psoriasis), and AGR regions (inverse psoriasis).
This study aimed to compare the immune and barrier features of psoriasis localized to SGP areas (psoriasis vulgaris) and psoriasis on SGR regions (scalp psoriasis), to determine if the immune milieu of healthy skin influences the immune characteristics and, consequently, the treatment of psoriasis on distinct skin regions.
Since psoriasis is a T helper (Th)1/Th17-mediated skin disorder (4), the current study investigated the Th1- and Th17-related immune and barrier alterations in lesional skin samples of patients with psoriasis vulgaris on SGP skin and scalp psoriasis (each n = 6) (Table SI) by immunohistochemistry and RT-qPCR (for details see Appendix S1).
Immunostaining of CD4+ T cells, CD11c+ myeloid dendritic cells (mDCs) and CD1a+ Langerhans cells (LCs) revealed no significant differences between psoriasis vulgaris on SGP skin and scalp psoriasis on SGR skin (Fig. S1).
Gene expression levels for Th1- and Th17-related cytokines, as interferon (IFN)γ, IL-12, IL-17 and IL-23 were similar (Table SII), and the protein levels of IFNγ, IL-17 and IL-23 were also similar between the 2 groups. No differences in the Th17-related chemokines, CCL2 and CCL20, were detected at the mRNA level (Table SII). In contrast, the protein expression of CCL20 was significantly higher in scalp psoriasis compared with psoriasis vulgaris of SGP skin (Table SII, Fig. S2).
Expression of the most common pro-inflammatory cytokines, IL-1β and tumour necrosis factor alpha (TNF-α), was investigated at the mRNA level, while immunostaining for TNF-α was also performed. Their expression at the mRNA level (Table SII) and TNF-α protein levels were similar in the 2 psoriatic sample groups (Table SII, Fig. S2).
To further investigate the Th17-related components of the innate immune response, this study assessed the gene expression levels of different AMPs (S100A7/8/9, human beta defensin (DEFB)4B, lipocalin (LCN)2), and protein levels for LCN2 and S100A8. There were no significant differences between the 2 psoriatic groups, at either gene or protein levels (Table SII, Fig. S3), except for the gene expression of LCN2, which was significantly higher in scalp psoriasis (Table SII).
Finally, the mRNA levels of key molecules involved in the formation and maintenance of the epidermal barrier (loricrin (LOR), filaggrin (FLG), keratin (KRT) 6, KRT17) were also examined by qPCR, while LOR, FLG, and KRT17 were evaluated, using immunohistochemistry. Expression of these molecules was similar in psoriasis samples from SGR and SGP skin, at both gene and protein levels (Table SII, Fig. S3).
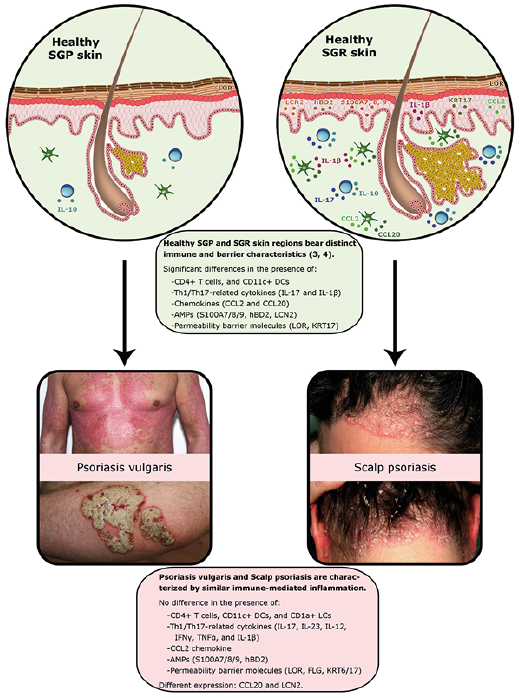
This study compared the immune characteristics of psoriasis vulgaris on SGP skin and scalp psoriasis on SGR skin to determine whether the inflammation developed in the 2 subtypes of psoriasis are influenced by the primarily distinct immune milieu of the different healthy skin areas. The results show that the mediators of both innate immune responses and Th1/Th17 type adaptive immune pathways were expressed similarly in scalp psoriasis and psoriasis vulgaris of SGP skin (Fig. 1). In addition, no significant differences could be detected in the expression of barrier molecules (Fig. 1). Significant differences were found only in LCN2 mRNA and CCL20 protein expression, with higher levels in scalp psoriasis. Since these parameters have previously been shown to be elevated even in healthy SGR skin compared with SGP (3), these differences may reflect the original immune characteristics of SGR skin region rather than psoriasis-related features (Fig. 1).
Fig. 1. Although the immune and barrier characteristics of healthy sebaceous gland poor (SGP) and sebaceous gland rich (SGR) skin are different, the psoriatic plaques developing on these distinct areas bear similar cellular, molecular and barrier characteristics. AMP: antimicrobial peptide; CCL: chemokine (C-C motif) ligand; hBD2: human beta defensin2; FLG: filaggrin; IFNG: interferon gamma; IL: interleukin; KR: keratin; LCN: lipocalin; LOR: loricrin; TNFA: tumour necrosis factor alpha.
The immune characteristics of psoriasis in different skin areas have been compared in a few publications (5–9), but only 2 publications have focused on comparing scalp psoriasis and psoriasis vulgaris (5, 6). The research focus and applied methods of these 2 studies were different from ours; furthermore, barrier components were not examined at the protein level (5, 6). Moreover, the conclusions of these 2 articles appear to be contradictory. In general, the results of the current study are in line with that of Ruano and colleagues (5), who, despite revealing some differences in the magnitude of dysregulation between the 2 forms of psoriasis by transcriptomic analyses, concluded that the immune mechanisms of scalp psoriasis are fundamentally similar to that of skin psoriasis (5). In another study, Ahn et al. concluded that distinct psoriasis subtypes display differences in IL-17, IFN-γ and IL-22 production (6). Although these results appear to be contrary to ours, these differences were significant only when palmoplantar psoriasis were compared with conventional plaque psoriasis (6). In another publication, chronic plaque psoriasis and inverse psoriasis, characteristic of AGR skin, were compared, and IL-17 was identified as their major shared pathway (9). These results support our findings showing that psoriasis localized to different skin areas share similar IL-17 related immune characteristics.
In clinical practice, the treatment of scalp psoriasis is considered more difficult than that of psoriasis vulgaris on SGP skin, since the high density of hair follicles and pilosebaceous units makes the application of local therapy and phototherapy technically complicated. Therefore, new formulations, such as foam or gel, were developed as new treatment modalities for this region (10). Clinical practice and studies show that biological treatments have the same efficacy for psoriasis vulgaris and scalp psoriasis (11). These findings are supported by the current study, showing that, in spite of the significant differences between healthy SGR and SGP skin immune milieu, psoriatic plaques developing on these distinct areas bear similar cellular, molecular, and barrier characteristics (Fig. 1). In summary, the results of this study suggest that, although the formulation of the local therapy needs to be different for psoriasis localized to the scalp vs SGP skin areas, there is no indication for the development of active ingredients with different mechanisms of action.
The publication is supported by NKFIH K-128250, GINOP-2.3.2-15-2016-00050 and EFOP-3.6.1-16-2016-00022 projects. The project is co-financed by the European Union and the European Regional Development Fund and the European Social Fund. This project was supported by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences (AK and DZ) and by the ÚNKP-18 4-DE-275 New National Excellence Program of the Ministry of Human Capacities”.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize