BOTULINUM TOXIN TYPE A IN THE HEALING OF ULCER FOLLOWING ORO-MANDIBULAR DYSKINESIA IN A PATIENT IN A VEGETATIVE STATE
Domenico Intiso, MD1, Mario Basciani, MD1, Filomena Di Rienzo, MD1, Maurizio Tolfa, MD1, Giuseppina Grimaldi, MD2 and Piero Fiore, MD2
From the 1Department of Neuro-Rehabilitation IRCCS “ Casa Sollievo della Sofferenza”, San Giovanni Rotondo (FG), and 2Department of Rehabilitation Medicine, University of Foggia, Foggia, Italy
OBJECTIVE: Use of botulinum toxin is expanding as clinical studies demonstrate new potential therapeutic applications. In rehabilitation, botulinum toxin is predominantly used as adjunct therapy for the treatment of spasticity, but it may prove useful for other atypical clinical situations.
Case history: A 73-year-old man had a severe sub-arachnoid haemorrhage following the rupture of a giant aneurism of the middle left cerebral artery. Clinically, the patient presented a vegetative state and an oro-mandibular dyskinesia that produced a chronic ulcer on the lower lip. As treatment for this dyskinesia, a total of 320 U botulinum toxin type A were injected into the upper and lower orbicularis oris and masseter muscles.
Results and Discussion: This treatment allowed for application of topical medication and subsequently, ulcer healing. Botulinum toxin type A may be an important therapeutic aid for clinicians faced with treating persistent pathological conditions caused by dyskinesia.
Key words: botulinum toxin type A, dyskinesia, ulcer, vegetative state, rehabilitation.
J Rehabil Med 2008; 40: 315–316
Correspondence address: Domenico Intiso, Department of Neuro-Rehabilitation, IRCCS “Casa Sollievo della Sofferenza”, Viale Cappuccini 1, IT-71013 San Giovanni Rotondo (FG), Italy. E-mail: d.intiso@operapadrepio.it
Submitted March 7, 2007; accepted January 22, 2008
Introduction
The use of botulinum toxin (BTX-A) is one of the most important developments in the therapeutics of movement disorders such muscular dystonia and dyskinesia (1). BTX-A, either alone or an adjunct to other agents, has also emerged as a new treatment option for a wide range of pathologies associated with gastroenterological and urological diseases, laryngeal dystonia and cosmetic treatments for ageing and trauma (2). In rehabilitation, BTX is predominantly used for the treatment of spasticity, prevention of contracture and bone dislocation, as well as for facilitating orthoses or cast application (3, 4). Another growing use of BTX is for the prevention of facial scar enlargement and the improvement of facial wound healing (5).
A new indication for BTX-A, as described in this case report, is in the treatment of an oro-mandibular dyskinesia that had led to a chronic, untreatable lower lip ulcer in a subject with severe neurological dysfunction. This treatment allowed for the medication and eventual healing of the ulcer.
Case REPORT
A 73-year-old man presented with a sudden lack of consciousness and coma state. A brain computer tomography scan performed in the emergency room showed a severe sub-arachnoid haemorrhage following the rupture of a giant aneurism of the middle left cerebral artery. After prompt neurosurgical treatment, he was admitted to the intensive care unit for mechanical ventilation and artificial nutrition by balloon-tipped percutaneous endoscopic gastrostomy.
On admission to the rehabilitation ward, the patient was in a vegetative state: he was not responsive and showed a slight asymmetric flexion response of the arms to painful stimulation. His limbs were positioned in hip adduction and mild flexion to knee due to contracture of the ischio-crural muscles. The patient also presented oro-mandibular dyskinesia consisting of inflexion and sucking of the lower lip, forced jaw and upper lip closing and repetitive sucking and jawing. The subject had no teeth and the involuntary repetitive movement produced a circular skin ulcer located on the inferior external edge of the lower lip (Fig. 1). The ulcer had slightly irregular borders and was graded as stage II–III according to the European Pressure Ulcer Advisory Panel wound classification system (6). Because of this dyskinetic movement disorder, all efforts at healing the ulcer by topical medication had failed. Treatment of the oro-mandibular dyskinesia was attempted in order to reduce the strength of mouth closure and to weaken the inflexion and sucking of the lower lip to allow for medication of the ulcer.
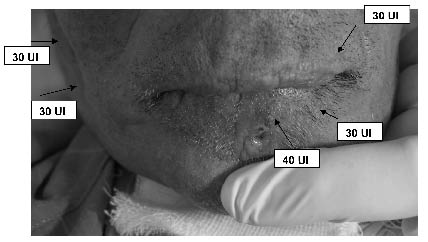
The orbicularis oris muscle was treated with a total of 200 IU BTX-A (Dysport®, Ipsen Limited, Slough, UK): the superior right and left (30 IU twice) and inferior right and left (30 IU twice) peripheralis orbicularis and the lower right and left orbicularis marginalis (40 IU twice) components. The inferior and superior parts of masseter muscle on both the right and left sides were treated with 30 IU of BTX-A, for a total of 120 IU per session (Fig. 1). Thus, a total of 320 IU BTX-A were administered in one sitting. Electromyographic guidance was not used, since orbicularis and masseter muscles are easily visible.
Fig. 1. Small, circular ulcer (II–III stage) of the lower lip was formed due to dyskinetic oral muscle movements following severe cerebral haemorrhage. Arrows: infiltration points and botulinum toxin type A dose used for each site of injection in both the upper and lower orbicularis and masseter muscles.
A month from the first BTX-A treatment, the dyskinetic disorder had improved. The strength of mouth closure was decreased and contraction in the inflexion and sucking of the lower lip were reduced. It was then possible to apply topical hydrocolloid and polyurethane hydrogel products for treatment of the ulcer. A second infiltration with the same BTX-A dosage (320 IU total) was performed after 2 months to maintain weakness of orbicularis and masseter muscles and to promote complete ulcer healing. The treatment further reduced the sucking and forced mouth closure, allowing for care of the ulcer, which 3 months from the initial infiltration, had healed completely (Fig. 2).
Fig. 2. Ulcer healing after 2 botulinum toxin type A (Dysport®) infiltrations of 320 units per single session.
Discussion
A vegetative state often occurs after dramatic cerebrovascular events result in extensive brain tissue damage. The rehabilitation process of these patients involves clinicians, nurses and caregivers, who must fulfil complex and challenging tasks using a multidisciplinary approach. The present case history describes the successful use of BTX-A in the treatment of a chronic, untreatable ulcer caused by an oro-mandibular dyskinesia resulting from a severe cerebral haemorrhage.
The use of BTX-A is increasing with the publishing of studies that demonstrate new clinical indications (2). A growing use of BTX has recently emerged for the prevention of facial scar widening and for the improvement of facial wound healing in patients undergoing plastic reconstruction (7). Local injection of BTX leads to immobilization of traumatic forehead lacerations, resulting in enhanced wound healing and less noticeable scars (7, 8). On the basis of these reports and its well-known muscular weakening activity, it was thought that BTX-A injections could decrease the movement disorder and improve lip ulcer healing in the reported patient. Results showed that BTX-A treatment reduced the forced closure of the mouth and weakened orbicularis oris muscles and repetitive sucking, permitting the topical medication of ulcer. In a rehabilitation setting, adjunct to physical therapy and other interventions, the injection of BTX-A to weaken overactive muscles can provide a window of opportunity to improve some of the complex clinical deficits and disorders affecting patients in need of rehabilitative treatment. The complexity of neurological and functional abnormalities of patients who undergo rehabilitation demands an integrated approach tailored to the specific needs of the patients over time. In the case described here, the involuntary repetitive forced oro-mandibular dyskinesia produced an ulcer of the lower lip that did not heal by common therapeutic interventions because constant movement precluded topical application of medication. To our knowledge, this is the first report on the use of BTX for dyskinetic oral movements and associated ulcer. Some may consider that treatment is unnecessary, given the site and size of the ulcer is of little impact in a patient in a vegetative state. However, we consider it important to strive to attain the best clinical and functional benefit that might improve the quality of care of patients undergoing rehabilitation. In conclusion, BTX-A might be a useful adjunct to interventions in the treatment of dyskinesia that evokes difficult to treat pathological sequelae.
References
1. Papapetropoulos S, Singer C. Botulinum toxin in movement disorders. Seminar Neurol 2007; 27: 183–194.
2. Pullman SL. The myriad uses of botulinum toxin. Ann Intern Med 2005; 143: 838–839.
3. Turkel CC, Bowen B, Liu J, Brin MF. Pooled analysis of the safety of botulinum toxin type A in the treatment of post-stroke spasticity. Arch Phys Med Rehabil 2006; 87: 786–792
4. Bjornson K, Hays R, Graubert C, Price R, Won F, McLaughlin JF, Cohen M. Botulinum toxin for spasticity in children with cerebral palsy: a comprehensive evaluation. Pediatrics 2007; 120: 49–58
5. Wilson AM. Use of botulinum toxin type A to prevent widening of facial scars. Plast Reconstr Surg 2006; 117: 1758–1766.
6. European Pressure Ulcer Advisory Panel. Available at: www.epuap.org/grading.htm
7. Gassner HG, Brisset AE, Otley CC, Boahene DK, Boggust AJ, Weaver AL, et al. Botulinum toxin to improve facial wound healing: a prospective, blinded, placebo-controlled study. Mayo Clin Proc 2006; 81: 1023–1028.
8. Hegedus F, Diecidue R, Taub D, Nyirady J. Non surgical treatment modalities of facial photodamage: practical knowledge for the oral and maxillofacial professional. Int J Oral Maxillofac Surg 2006; 35: 389–398.