
1Rehabilitation Medicine, Changi General Hospital, 529889 Singapore
2Spinal Injury Rehabilitation Centre, Pinderfields General Hospital, Pinderfields, WF1 4DG, United Kingdom
Objective: Sacral insufficiency fractures should be considered in differential diagnosis as a cause of autonomic dysreflexia and other vague symptoms in patients with spinal cord injury.
Setting: The Supra Regional Tertiary Centre, Midlands Centre for Spinal Injuries, Oswestry, UK.
Method: Outpatient clinic review of 2 patients with long-standing spinal cord injury presenting with vague symptoms of abdominal discomfort, and increased spasms including autonomic dysreflexia in which no evidence of causation was found on clinical examination.
Result: Radiological investigation with computed tomography of the abdomen and pelvis demonstrated sacral insufficiency fractures in both cases. These were managed conservatively and, following a diagnosis of osteoporosis, treatment with bisphosphonates was commenced. There was an improvement in symptomatology at the 12-week follow-up.
Conclusion: Longevity in spinal cord injury continues to improve with increased awareness and improved management. However, along with improved longevity, secondary complications may occur, including sacral insufficiency fracture, which is difficult to diagnose and can affect quality of life. An awareness of sacral insufficiency fracture and its possible occurrence as a differential diagnosis in patients with chronic spinal cord injury presenting with vague symptoms can result in early diagnosis. Conservative management with bed rest is a viable option.
Key words: spinal cord injury; sacral insufficiency fracture; autonomic dysreflexia; computed tomography of the abdomen and pelvis; bisphosphonates.
Longevity in patients with spinal cord injury continues to improve with increased awareness and improved management. However, along with improved longevity secondary complications may occur, including sacral insufficiency fracture, which is difficult to diagnose and can affect quality of life. An awareness of sacral insufficiency fractures and their possible occurrence as a differential diagnosis in patients with chronic spinal cord injury presenting with vague symptoms can result in early diagnosis. Conservative management with bed rest is a viable option.
Accepted Sep 4, 2019; Published Oct 4, 2019
JRM-CC 2019; 2: 1000019
Correspondence address: Kappaganthu Venkatesh Prasanna, Rehabilitation Medicine, Changi General Hospital, 529889 Singapore. E-mail: vkprasanna@hotmail.com
Sacral insufficiency fracture (SIFs) have been well reported since their first description by Lourie in 1982 (1). This is a known condition in middle-aged women, and may be associated with underlying osteoporosis. Presentation of SIFs in patients with spinal cord injury (SCI) can be variable due to the lack of sensation below the level of the SCI. Clinical manifestation may be the first sign of a SIF. Knowledge of SIF is important in order to establish the diagnosis and further management of this condition. We report here 2 unusual cases of SIFs, which were incidentally diagnosed in male patients with long-standing SCI, and their management, along with a literature review.
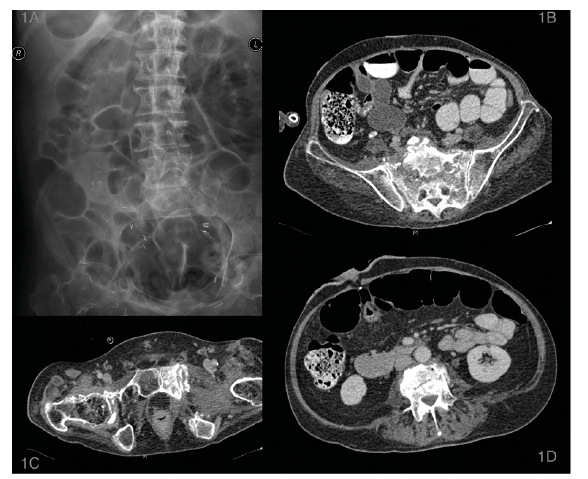
A 59-year-old man with C5 Frankel A tetraplegia for 35 years with no history of drug or alcohol abuse, presented to the outpatient spine clinic with an altered bowel pattern, increased spasms, sweating and increased frequency of autonomic dysreflexia. Examination revealed tachycardia, elevated blood pressure with sweaty and clammy peripheries. His abdomen was noted to be soft, non-tender, with slight distension and normal bowel sounds. There was no evidence of neurological deterioration, fractures or pressure sores. A plain abdominal and pelvic radiograph showed prominent loops of gaseous bowel (Fig. 1). A computed tomography (CT) scan of the abdomen and pelvis was performed to further evaluate his abdominal symptoms, and incidentally picked up a sacral fracture with no other remarkable findings. A bone mineral density test was performed, which suggested osteoporosis (Z score–3.2 in the femoral neck). Symptoms of autonomic dysreflexia abated with hydration, and analgesia and adequate bowel clearance. The SIF was managed with bed-rest for 6 weeks and the patient was commenced on bisphosphonates. At 12-week follow-up the patient was reported to be well with no abdominal symptoms, pain or spasms.
Fig. 1. Case 1: A) Plain abdominal x-ray showing the prominent loops of bowel usually masking detection of sacral fracture. B) Computed tomography(CT) showing sacral insuffciency fracture extending into the sacral canal, Denis type 2 fractures bilaterally. C) CT scan of the same patient showing incidental old healed pubic symphysis pubic rami fracture, D) CT scan of the same patient showing old healed incidental L4 lumbar spine fracture.
A 52-year-old man with traumatic SCI – C6 Frankel A, for 34 years, felt a clunk whilst caregivers were getting him out of bed. Following this he had increased pain in the shoulder blades, frequent episodes of autonomic dysreflexia and increased spasms. A co-incidental urinary tract infection was thought to be causative and was treated with antibiotics with little response. Plain radiographs of the sacrum and pelvis did not reveal any obvious fracture. A bone scintigraph, as advised by the radiologist, revealed a high uptake bilaterally in the sacrum and pubis (Fig. 2). Subsequent CT scan confirmed a SIF extending into the posterior iliac crest on the left side. In addition, there were bilateral pubic bone fractures with generalized osteopaenia. He was commenced on intravenous zolendronate.
Fig. 2. Case 2: A) Bone scintigraphy showing classic ”H” sign confirming increasing uptake bilateral sacral ala and pubic rami. B) CT scan showing bilateral sacral fractures extending into zone2 and 3of sacrum (as per Denis classfication). C) CT scan of the same patient showing bilateral old healed pubic rami fractures with old per trochanteric fracture of left hip.
SIFs occur most commonly in women aged > 55 years whose bone strength is inadequate to withstand normal repetitive stress (2, 3). Several conditions can predispose to SIFs: postmenopausal osteoporosis being one of the main causes. Also, the long-term use of steroids, radiation therapy, hyperparathyroidism, osteomalacia, renal osteodystrophy, rheumatoid arthritis, anticonvulsant therapy, Cushing’s syndrome, primary biliary cirrhosis, and myelomatous disorders, which can lead to secondary osteoporosis, may all contribute indirectly to SIFs (2).Patients with SCI respond to noxious stimuli differently from able-bodied individuals, as a result of diminished or absent sensation below the level of spinal injury. These patients manifest their symptoms as secondary complications of SCI, namely increased spasms, exaggerated neuropathic pain, chronic constipation and/or frequent episodes of autonomic dysreflexia (4, 5).
According to the Denis classification (2, 3) (Fig. 3), most SIFs are located within Zone 1 of the sacral body, in contrast to traumatic fractures that occur in Zone 2 along the sacral foramina. SIFs are usually vertical and parallel to the sacroiliac joint away from the sacral foramina; neurological deficits are therefore unusual (2). SIFs are usually bilateral and likely to be connected by a horizontal fracture through the upper sacral body (3). Associated fractures are seen in 25–80% of patients with SIFs, most common being pubic rami fractures followed by vertebral compression fractures, iliac wing fractures and inter-trochanteric fractures (2, 3).
Fig. 3. Denis classification of sacral fractures.
Plain radiographs, are usually inconclusive (2, 3, 6). Diagnosis based on plain radiograph alone was correct in only 12% of cases from this case series (2). Technetium bone scan is highly sensitive and is able to detect occult fractures of the pelvic ring (2). The classical “H” sign, along with variants, can be useful in detecting SIFs (2, 6). However, this lacks specificity, as infection and metastatic disease can also mimic this sign. CT is regarded as the gold standard in diagnosing these fractures (2, 6). A false-negative result of up to 25% of cases was reported with CT. Magnetic resonance imaging (MRI) has a sensitivity of 100%, but specificity in this study was found to be 83% (2, 6).
A combination of bone scintigraphy and CT or MRI has a greater chance of detecting these fractures (2, 6). These patients tend to have severe osteoporosis. It is recommended to treat them with bisphosphonates for up to 2 years (2).
Laboratory data are usually unremarkable. In the presence of reversible causes of secondary osteoporosis, such as hyperthyroidism, hyperparathyroidism or osteomalacia; however, the presence of sacral stress fractures should be considered (7). Levels of thyroid-stimulating hormone (TSH), parathyroid hormone (PTH), calcium, phosphorus, albumin, 25-hydroxyvitamine D, urinary calcium, creatinine, full-blood count, liver function tests, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) must be investigated if secondary osteoporosis is suspected (7).
Serum levels of alkaline phosphatase (ALP), a marker of bone formation, are often slightly raised, and this should lead clinicians to consider a differential diagnosis between stress fractures and an active form of Paget’s disease (7).
The first step in the treatment of sacral stress fractures is pain control. A variety of analgesics that act centrally, such as paracetamol and opioids, are available in clinical practice and should be used until the pain resolves (7). There are reasons for concern about the use of peripherally acting analgesics (non-steroidal anti-inflammatory drugs; NSAIDs) in fracture healing, because they block the activity of prostaglandins, especially prostaglandin E2 (PGE2), which plays a significant role in bone healing (7). Vitamin D deficiency is a relatively common finding in elderly people (7). In the case of sacral fracture, a condition of vitamin D insufficiency must be suspected, and an oral supplement of calcium and vitamin D should be prescribed (7). Patients with SCI are at higher risk of immobility and osteoporosis, and hence mobilizing the patient, weight-bearing exercises, physiotherapy and pharmacological management of osteoporosis are crucial in the management of SIFs.
Conclusion
Patients with long-standing SCI present with a wide variety of symptoms and signs, which can mask the underlying diagnosis. Vague symptoms of increased spasms, dysreflexia, bladder and bowel problems need thorough clinical examination and appropriate investigations. We recommend that SIFs are considered as a differential disgnosis in patients with long-standing SCI irrespective of their age. A combination of bone scintigraphy and CT or MRI is helpful to confirm the diagnosis. Conservative management remains a viable option, with good resolution of symptoms and improved quality of life.


 Click to show fullsize
Click to show fullsize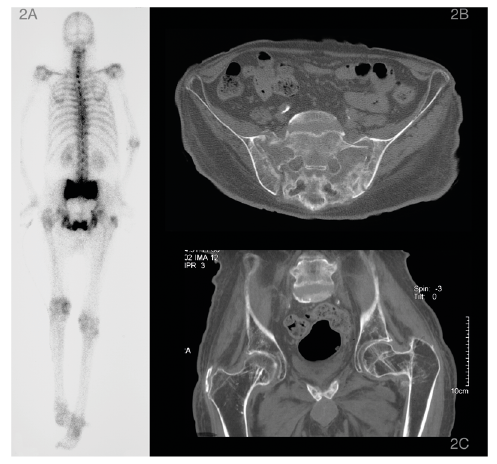 Click to show fullsize
Click to show fullsize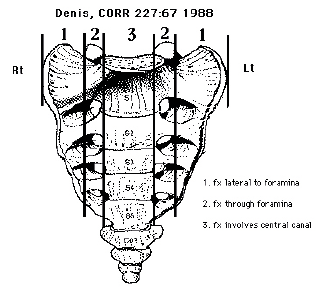 Click to show fullsize
Click to show fullsize